
Systemic Pathology — MCQs

On this page
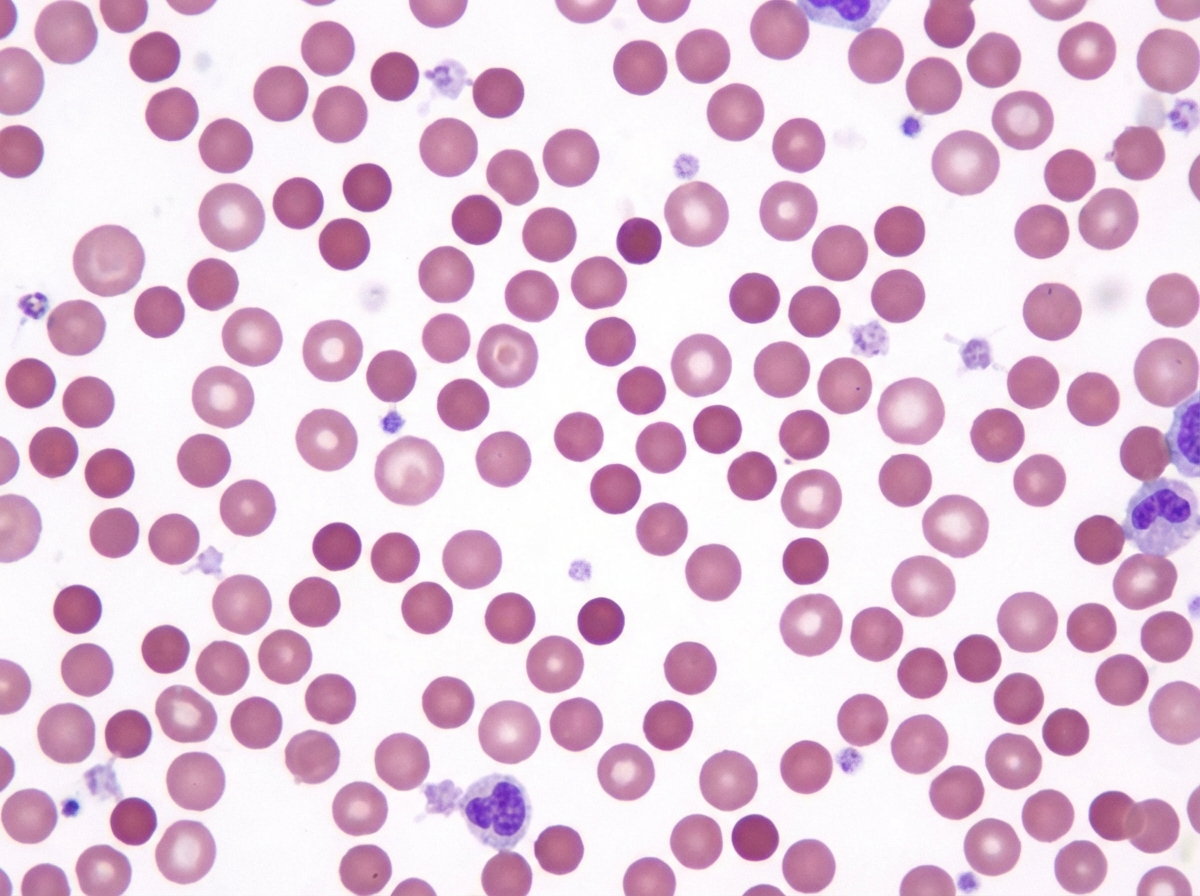
A 27-year-old woman presented to the clinic with recurrent abdominal swelling and stunted growth relative to her siblings. She has a history of multiple blood transfusions in her childhood. She has a family history of jaundice in her father who was operated on for multiple gallbladder stones. The physical examination reveals a pale, icteric, small and short-statured young lady. On abdominal examination, the spleen was enlarged by 6 cm below the left costal margin, but the liver was not palpable. The ultrasound of the abdomen reveals multiple gallbladder stones. The laboratory test results are as follows: Hb 9 g/dL Hct 27% WBC 6,200/mm3 Platelets 200,000/mm3 MCV 75 um3 MCHC 37 gm/dL Reticulocytes 6.5% A peripheral blood smear is presented in the image. The direct Coombs test was negative. The osmotic fragility test was increased. What is the most likely cause of her condition?
A 9-year-old boy is brought to the physician by his mother because of a 3-day history of fever and bleeding after brushing his teeth. His mother also reports that her son has asked to be picked up early from soccer practice the past few days because of fatigue. He appears pale and ill. His temperature is 38.3°C (101.1°F), pulse is 115/min, and blood pressure is 100/60 mm Hg. The lungs are clear to auscultation. Examination shows a soft, nontender abdomen with no organomegaly. There are several spots of subcutaneous bleeding on the abdomen and shins. Laboratory studies show a hemoglobin concentration of 7 g/dL, a leukocyte count of 2,000/mm3, a platelet count of 40,000/mm3, and a reticulocyte count of 0.2%. Serum electrolyte concentrations are within normal limits. A bone marrow biopsy is most likely to show which of the following findings?
A 46-year-old woman presents to your office with oral lesions as shown in Image A. On examination, you find that her back has flaccid bullae that spread when you apply lateral pressure with your fingertips. This patient most likely has autoantibodies directed against which of the following?

A 12-year-old boy is found on a routine auditory screening to have mild high frequency hearing impairment. On exam, he has no ear pain, no focal neurological deficits, and no cardiac murmurs. He has not had any recent illness. Laboratory studies show: Serum: Creatinine: 0.7 mg/dl Protein: 3.8 g/dl Antistreptolysin O titer: 60 Todd units (12-166 normal range) Urinalysis: Microscopic heme Protein: 4+ RBCs: 6/hpf A kidney biopsy is taken. Which of the following findings is most characteristic of this patient’s disease?
A 55-year-old female presents with pain in both hands and wrists for the past several years. It is associated with morning stiffness that lasts for almost an hour. Physical examination reveals tenderness and swelling in both hands and wrists, most severe over the proximal interphalangeal joints. Laboratory investigation reveals the presence of anti-cyclic citrullinated peptide (anti-CCP). Which of the following immune-mediated injuries is responsible for this patient’s condition?
A 7-year-old boy is brought to the emergency department by his parents with a 2-day history of severe fatigue. His parents say that he has no past medical history, but caught an illness that was going around his school 1 week ago. While ill, he had several days of abdominal pain and bloody diarrhea. His family history is significant for several family members who required blood transfusions, and he lives in an old house. Physical exam reveals conjunctival pallor and mild jaundice. Which of the following would most likely be seen on peripheral blood smear in this patient?
A healthy 29-year-old woman comes to the doctor because of recurrent episodes of bleeding from the nose and gums during the past week. These episodes occur spontaneously and resolve with compression. She also had 1 episode of blood in the urine 2 days ago. Examination shows punctate, nonblanching, reddish macules over the neck, chest, and lower extremities. Her leukocyte count is 8,600/mm3, hemoglobin concentration is 12.9 g/dL, and platelet count is 26,500/mm3. A peripheral blood smear shows a reduced number of platelets with normal morphology. Evaluation of a bone marrow biopsy in this patient is most likely to show which of the following findings?
A 12-year-old boy, otherwise healthy, presents with frequent nosebleeds and lower extremity bruising. His mother reports that his symptoms started about 2 weeks ago and have not improved. The patient received the Tdap vaccine 2 weeks ago. He has no current medications. The review of systems is significant for the patient having a stomach ache after winning a hamburger eating competition 2 weeks ago. The vital signs include: temperature 37.0°C (98.6°F), blood pressure 110/75 mm Hg, pulse 95/min, respirations 15/min, and oxygen saturation 99% on room air. On physical exam, the patient is alert and cooperative. The cardiac exam is normal. The lungs are clear to auscultation bilaterally. The lower extremities findings are shown in the image. Laboratory results return showing a platelet count of 18,000/µL, hemoglobin 13.2 g/dL, normal renal function, normal urinalysis, and normal coagulation studies. Which of the following best describes the pathogenesis of this patient's condition?

A 68-year-old woman is being evaluated for fatigue during a follow-up visit after implantation of a prosthetic aortic valve a month ago. She reports she has been feeling more tired than usual but associates it with her recent surgery. A complete blood count (CBC) reveals a hemoglobin of 9.5 g/dL and a reticulocyte percentage of 2.8%. Additionally, the serum haptoglobin is decreased while the platelet count is within the normal range. The patient is suspected to have a type of hemolytic anemia secondary to her prosthetic heart valve. Which of the following will most likely be seen in this patient's blood smear?
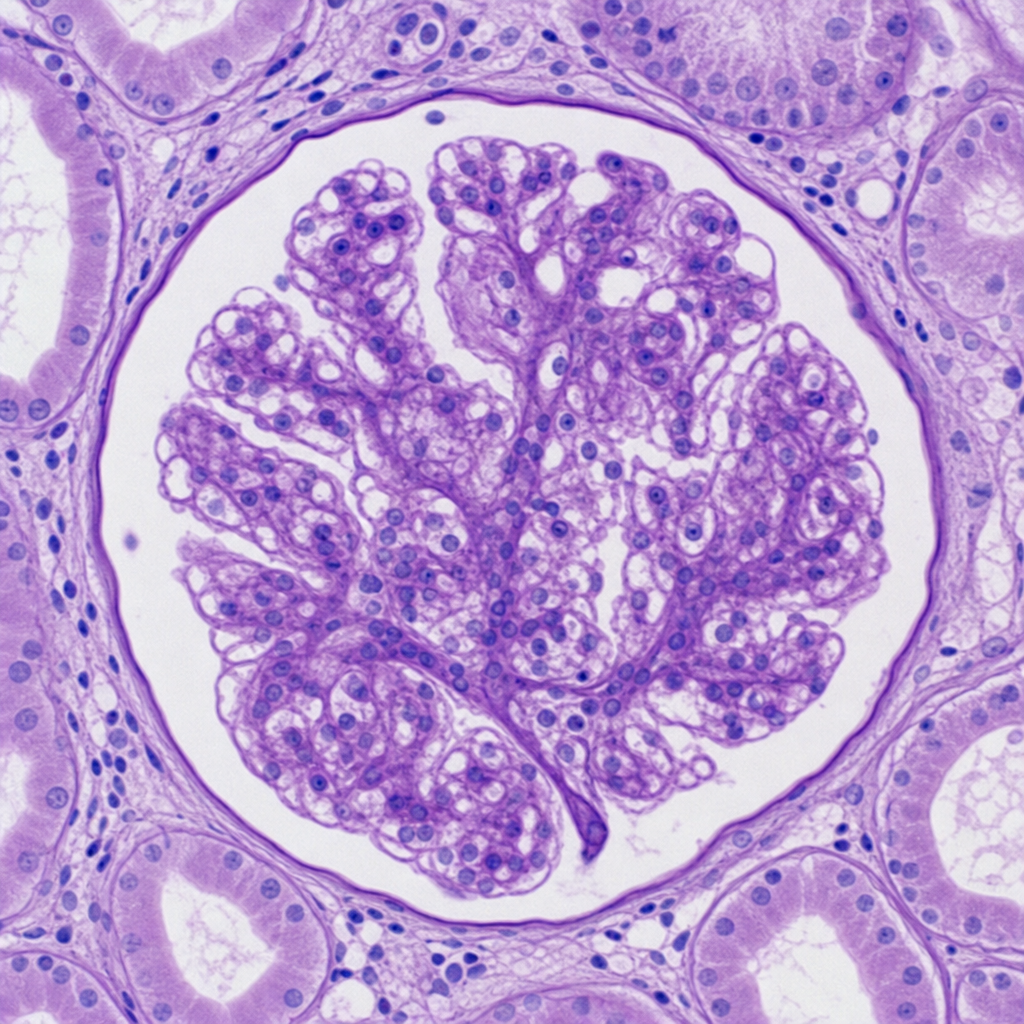
A 32-year-old African American woman presents to the office with complaints of frothy urine and swelling of her body that started 4 days ago. She noticed the swelling 1st in the face then gradually involved in other parts of her body. The frequency of urination is the same with no noticeable change in its appearance. She is human immunodeficiency virus (HIV) positive and is currently under treatment with abacavir, dolutegravir, and lamivudine. The vital signs include blood pressure 122/89 mm Hg, pulse 55/min, temperature 36.7°C (98.0°F), and respiratory rate 14/min. On physical examination, there is generalized pitting edema. Urinalysis results are as follows: pH 6.6 Color light yellow Red blood cell (RBC) count none White blood cell (WBC) count 1–2/HPF Protein 4+ Cast fat globules Glucose absent Crystal none Ketone absent Nitrite absent 24 hours of urine protein excretion 5.2 g HPF: high-power field A renal biopsy is performed which shows the following (see image). What condition is this patient most likely suffering from?
Practice by Chapter
Liver pathology (hepatitis, cirrhosis)
Practice Questions
Gallbladder and biliary tract disorders
Practice Questions
Pancreatic diseases
Practice Questions
Kidney diseases
Practice Questions
Male reproductive pathology
Practice Questions
Female reproductive pathology
Practice Questions
Breast pathology
Practice Questions
Endocrine pathology
Practice Questions
Bone and joint pathology
Practice Questions
Skeletal muscle diseases
Practice Questions
Peripheral nerve disorders
Practice Questions
Soft tissue tumors
Practice Questions
Head and neck pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app