
Systemic Pathology — MCQs

On this page
A 63-year-old man is brought to the emergency department by the police after he was found in the streets lying unconscious on the ground. Both of his pupils are normal in size and reactive to light. There are no obvious signs of head trauma. The finger prick test shows a blood glucose level of 20 mg/dL. He has been brought to the emergency department due to acute alcohol intoxication several times. The vital signs include: blood pressure 100/70 mm Hg, heart rate 110/min, respiratory rate 22/min, and temperature 35℃ (95℉). On general examination, he is pale looking and disheveled with an odor of EtOH. On physical examination, the abdomen is soft and non-tender with no hepatosplenomegaly. After giving a bolus of intravenous dextrose, thiamine, and naloxone, he spontaneously opens his eyes. Blood and urine samples are drawn for toxicology screening. The blood alcohol level comes out to be 300 mg/dL. What will be the most likely laboratory findings in this patient?
A 4-year-old boy presents to the emergency department with a 1 hour history of severe knee pain after he bumped his knee against a door. He has no past medical history though his parents say that he seems to bruise fairly easily. His parents say that they are afraid he may have accidentally taken his grandfather's warfarin medication. On presentation, he is found to have an erythematous, warm, swollen knee. Based on this presentation, a panel of laboratory tests are ordered with the following results: Bleeding time: 3 minutes Prothrombin time (PT): 12 seconds Partial thromboplastin time (PTT): 56 seconds Mixing studies show correction of the PTT Which of the following is most likely the cause of this patient's symptoms?
A previously healthy 17-year-old boy is brought to the emergency department by his mother for further evaluation after elective removal of his wisdom teeth. During the procedure, the patient had persistent bleeding from the teeth's surrounding gums. Multiple gauze packs were applied with minimal effect. The patient has a history of easy bruising. The mother says her brother had similar problems when his wisdom teeth were removed, and that he also has a history of easy bruising and joint swelling. The patient takes no medications. His temperature is 37°C (98.6°F), pulse is 90/min, and blood pressure is 108/74 mm Hg. Laboratory studies show: Hematocrit 35% Leukocyte count 8,500/mm3 Platelet count 160,000/mm3 Prothrombin time 15 sec Partial thromboplastin time 60 sec Bleeding time 6 min Fibrin split products negative Serum Urea nitrogen 20 mg/dL Creatinine 1.0 mg/dL Bilirubin Total 1.0 mg/dL Direct 0.5 mg/dL Lactate dehydrogenase 90 U/L Peripheral blood smear shows normal-sized platelets. Which of the following is the most likely diagnosis?
A 34-year-old man presents with acute-onset fever and weakness followed by shifting neurologic deficits (aphasia, motor deficits), which have lasted for a few days. His relatives add that his quantity of urine has reduced significantly over the last few days. He has never had any similar symptoms. Laboratory findings are significant for the following: Hb 8.6 g/dL WBC 6.5 × 1000/mm3 Platelets 43 × 1000/mm3 Cr 3.1 mg/dL BUN 25 mg/dL Na+ 136 mg/dL K+ 4.2 mg/dL Cl- 101 mg/dL HCO3- 24 mg/dL Glu 101 mg/dL Examination of the peripheral smear shows the presence of schistocytes, helmet cells, and spherocytes. Which of the following is true regarding this patient's condition?
A 43-year-old woman comes to the office with a 5-day history of a rash. She's had a rash across her neck, shoulders, and the palms of her hands for the past five days. She's also had large-volume watery diarrhea for the same period of time. Past medical history is notable for acute myeloid leukemia, for which she received a stem cell transplant from a donor about two months prior. Physical exam reveals a faint red maculopapular rash across her neck, shoulders, and hands, as well as an enlarged liver and spleen. Labs are notable for a total bilirubin of 10. Which of the following is the mechanism of this patient's pathology?
A 29-year-old African American woman presents with incidentally noted bilateral hilar lymphadenopathy on a recent chest radiograph for the evaluation of pneumonia 1 month earlier. Upon questioning, she reports a cough and dyspnea. The report provided by a previous ophthalmologic consultation did not demonstrate any eye abnormalities. Clinical laboratory pathologic analysis reveals an elevated level of angiotensin-converting enzyme. Her physical examination reveals no obvious abnormalities. Her vital signs show a heart rate of 76/min, respiratory rate of 16/min, and blood pressure of 123/73 mm Hg. Of the following options, which is the mechanism of the reaction causing hilar adenopathy in this patient?
A 47-year-old woman presents to her physician for difficulty swallowing. She states that she intentionally delayed seeing a physician for this issue. She says her primary issue with swallowing is that her mouth always feels dry so she has difficulty chewing food to the point that it can be swallowed. On physical examination, her oral mucosa appears dry. Both of her eyes also appear dry. Several enlarged lymph nodes are palpated. Which of the following patterns of reactive lymphadenitis is most commonly associated with this patient’s presentation?
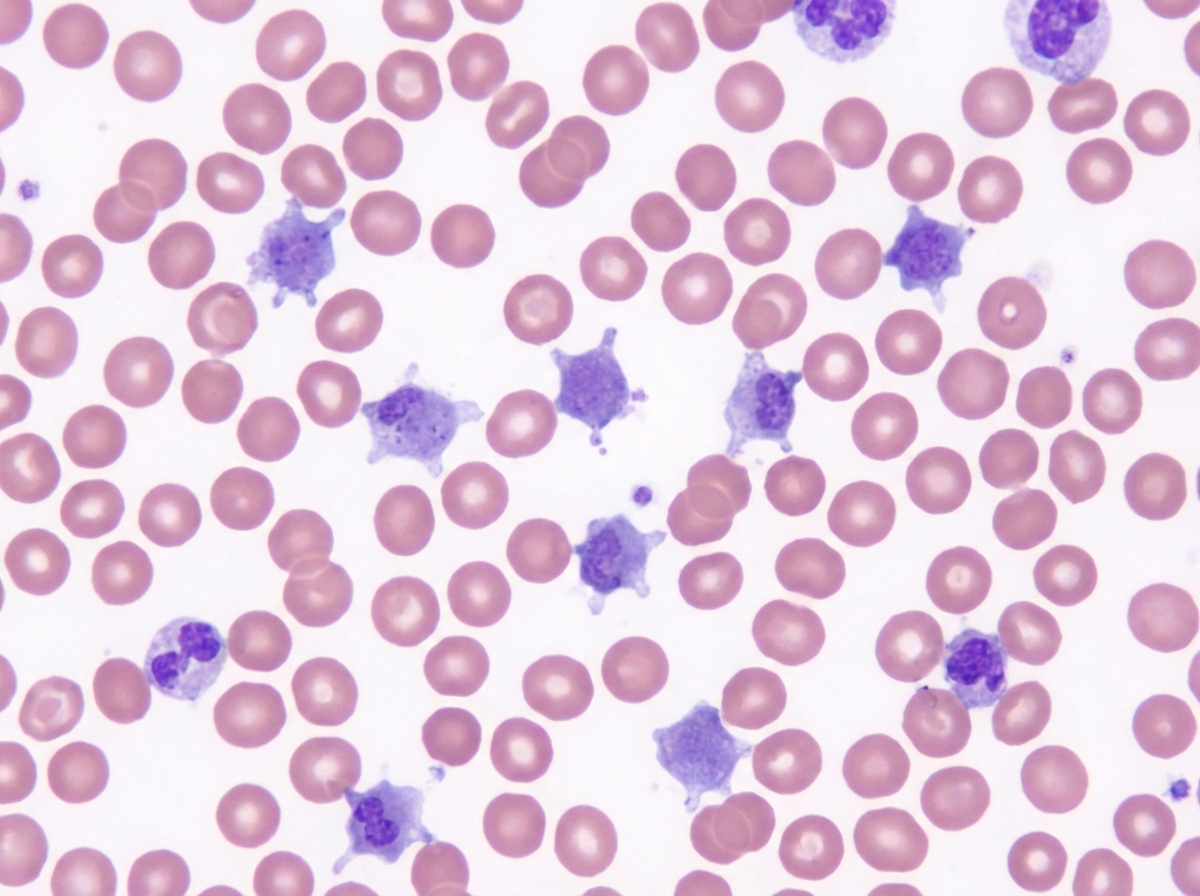
A 3-week-old boy is brought to the pediatrician by his parents for a circumcision. The circumcision was uncomplicated; however, after a few hours, the diaper contained blood, and the bleeding has not subsided. A complete blood count was ordered, which was significant for a platelet count of 70,000/mm3. On peripheral blood smear, the following was noted (figure A). The prothrombin time was 12 seconds, partial thromboplastin time was 32 seconds, and bleeding time was 13 minutes. On platelet aggregation studies, there was no response with ristocetin. This result was not corrected with the addition of normal plasma. There was a normal aggregation response with the addition of ADP. Which of the following is most likely true of this patient's underlying disease?
A 37-year-old man who had undergone liver transplantation 7 years ago, presents to the physician because of yellowish discoloration of the skin, sclera, and urine. He is on regular immunosuppressive therapy and is well-adherent to the treatment. He has no comorbidities and is not taking any other medication. He provides a history of similar episodes of yellowish skin discoloration 6–7 times since he underwent liver transplantation. Physical examination shows clinical jaundice. Laboratory studies show: While blood cell (WBC) count 4,400/mm3 Hemoglobin 11.1 g/dL Serum creatinine 0.9 mg/dL Serum bilirubin (total) 44 mg/dL Aspartate transaminase (AST) 1,111 U/L Alanine transaminase (ALT) 671 U/L Serum gamma-glutamyl transpeptidase 777 U/L Alkaline phosphatase 888 U/L Prothrombin time 17 seconds A Doppler ultrasound shows significantly reduced blood flow into the transplanted liver. A biopsy of the transplanted liver is likely to show which of the following histological features?
A 4-year-old male is evaluated for frequent epistaxis and mucous membrane bleeding. Physical examination shows diffuse petechiae on the patient’s distal extremities. Peripheral blood smear shows an absence of platelet clumping. An ELISA binding assay reveals that platelet surfaces are deficient in GIIb/IIIa receptors. Serum platelet count is normal. Which of the following is the most likely diagnosis?
Practice by Chapter
Liver pathology (hepatitis, cirrhosis)
Practice Questions
Gallbladder and biliary tract disorders
Practice Questions
Pancreatic diseases
Practice Questions
Kidney diseases
Practice Questions
Male reproductive pathology
Practice Questions
Female reproductive pathology
Practice Questions
Breast pathology
Practice Questions
Endocrine pathology
Practice Questions
Bone and joint pathology
Practice Questions
Skeletal muscle diseases
Practice Questions
Peripheral nerve disorders
Practice Questions
Soft tissue tumors
Practice Questions
Head and neck pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app