
Systemic Pathology — MCQs

On this page
A 51-year-old woman with Sjogren’s syndrome presents to her physician for suddenly developed palpitations. She feels more anxious than usual and has had difficulty sleeping well for the past 2 weeks. She has lost 2 kg (4.4 lb) since her last routine appointment 6 months ago. She also has had diarrhea and often feels like her heart is beating very quickly. On physical examination, her skin appears warm and moist. Her reflexes are hyperactive. Her thyroid is moderately enlarged and is non-tender. She has mild dry eyes and dry mouth. Her blood pressure is 136/88 mm Hg, pulse is 76/min, respirations are 17/min and temperature is 36.7°C (98.1°F). Which of the following pathologic findings is this patient likely to have?
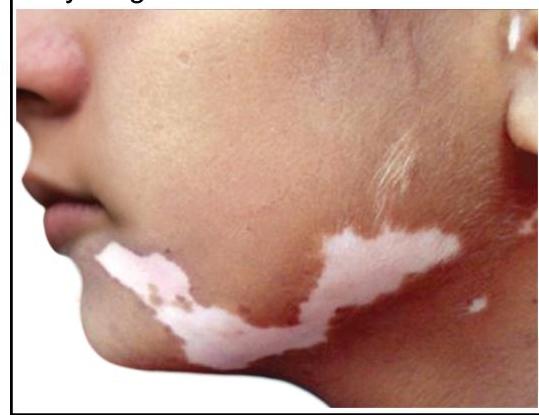
An otherwise healthy 17-year-old girl comes to the physician because of multiple patches on her face, hands, abdomen, and feet that are lighter than the rest of her skin. The patches began to appear 3 years ago and have been gradually increasing in size since. There is no associated itchiness, redness, numbness, or pain. She emigrated from India 2 years ago. An image of the lesions on her face is shown. Which of the following is most likely involved in the pathogenesis of this patient's skin findings?
An investigator is studying the outcomes of a malaria outbreak in an endemic region of Africa. 500 men and 500 women with known malaria exposure are selected to participate in the study. Participants with G6PD deficiency are excluded from the study. The clinical records of the study subjects are reviewed and their peripheral blood smears are evaluated for the presence of Plasmodium trophozoites. Results show that 9% of the exposed population does not have clinical or laboratory evidence of malaria infection. Which of the following best explains the absence of infection seen in this subset of participants?
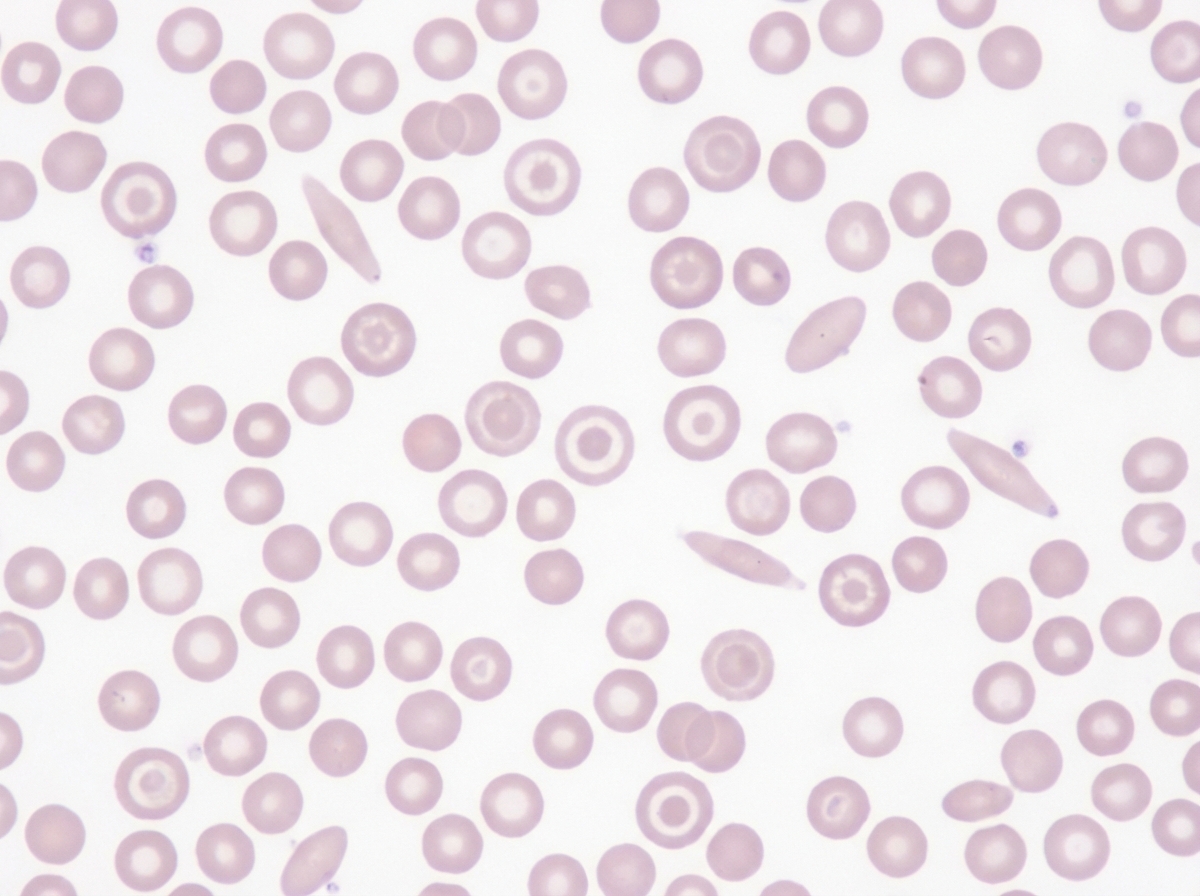
A 24-year-old Turkish female presents to your office for a routine examination. She recently started a new job and has been tired most of the time. She does not have any dizziness and has not lost consciousness. She follows a well-balanced diet and is not vegetarian. She has regular menstrual cycles with normal flow and denies any abnormal bleeding. She recalls that other family members have had similar symptoms in the past. On physical exam her temperature is 99°F (37.2°C), blood pressure is 115/78 mmHg, pulse is 100/min, respirations are 22/min, and pulse oximetry is 99% on room air. On physical exam, you notice conjunctival pallor. Labs are obtained and the results are shown below: Hemoglobin: 10.2 g/dL Hematocrit: 34% Leukocyte count: 5,000 cells/mm^3 with normal differential Platelet count: 252,000/mm^3 Mean corpuscular hemoglobin concentration: 20.4% Mean corpuscular volume: 65 µm^3 RBC count: 5.8 million/mm^3 RDW: 13.1% (normal) Ferritin: 68 ng/mL (normal) Hemoglobin electrophoresis: HbA2 4.8% (elevated) Peripheral blood smear is shown in the image provided. The cause of her anemia is most likely associated with which of the following?
A four-year-old boy is brought to his pediatrician by his mother for recurrent nosebleeds. The mother reports that the boy has had five nosebleeds within the past 2 weeks, each lasting between 15 and 20 minutes. The patient was born at term and has been hospitalized twice for pneumonia treatment. There is no family history of serious illness. The patient is at the 8th percentile for height and the 30th percentile for weight. Vital signs are within normal limits. Examination shows a small, thin child with two flat, dark brown areas of hyperpigmentation across the upper back and a similar discoloration on the left buttock. There is bilateral esotropia. Laboratory studies show a hemoglobin concentration of 9.3 g/dL, mean corpuscular volume of 107 μm3, leukocyte count of 3,800/mm3, and platelet count of 46,000/mm3. Which of the following is the most likely underlying cause of this patient's condition?
A 29-year-old woman presents with shortness of breath and chest pain for the past week. She says her chest pain is aggravated by deep breathing and she becomes short of breath while walking upstairs in her home. She also has been feeling feverish and fatigued for the past week, as well as pain in her wrists, hands, and left knee. Review of systems is significant for a 4.5 kg (10.0 lb) weight loss over the previous month. Past medical history consists of 2 spontaneous abortions, both of which occurred in the 1st trimester. On physical examination, there is a pink rash present over her face, which is aggravated by exposure to sunlight. There are decreased breath sounds on the right. A chest radiograph is performed which reveals evidence of a right pleural effusion. Serum ANA and anti-dsDNA autoantibodies are positive. Urinalysis is unremarkable. Errors with which of the following is most likely to lead to her disease?
A 51-year-old African American man presents to his primary care physician’s office for an annual visit. He has no major concerns and says that he has been healthy for the last year. His past medical history is significant for diabetes as well as long standing hypertension that has developed gradually since his 30's; however, he has refused to take any medications. Physical exam shows no abnormal findings. Routine laboratory testing reveals the following: Serum creatinine concentration: 1.5 mg/dL Blood urea nitrogen: 31 mg/dL Based on these results, urine studies are conducted that reveal mild proteinuria of less than 1 g/day and no casts. Which of the following is most likely associated with the cause of this patient's elevated creatinine?
A 35-year-old man presents with acute onset of chest pain, trouble breathing, and abdominal pain. He says he had recently been training for a triathlon competition when, over the past week, he noticed that he was getting more tired than usual. He figured that it was due to his age since most of the people training with him were in their 20s. However, after completing a particularly difficult workout over this last weekend he noticed left-sided chest pain that did not radiate, and abdominal pain, worse on the right side. The pain persisted after he stopped exercising. This morning he noticed red urine. The patient reports similar past episodes of red urine after intense exercise or excessive alcohol intake for the past 5 years, but says it has never been accompanied by pain. Past medical history is significant for a urinary tract infection last week, treated with trimethoprim-sulfamethoxazole. Physical examination is significant for a systolic flow murmur loudest at the right upper sternal border and right upper quadrant tenderness without guarding or rebound. Laboratory findings are significant for the following: Hemoglobin 8.5 g/dL Platelets 133,000/µL Total bilirubin 6.8 mg/dL LDH 740 U/L Haptoglobin 25 mg/dL An abdominal MRI with contrast is performed which reveals hepatic vein thrombosis. Which of the following laboratory tests would most likely to confirm the diagnosis in this patient?
A 29-year-old woman comes to the clinic for complaints of fatigue and palpitations for the past 3 days. She reports that even standing up and walking around takes “a lot of energy.” She was forced to call in sick today to her work as a kindergarten teacher. She denies any previous episodes but does endorse symmetric joint pain of her hands, wrists, knees, and ankles that was worse in the morning over the past week that self-resolved. She also reports a runny nose and congestion. Past medical history is unremarkable. Physical examination demonstrates splenomegaly, pallor, and generalized weakness; there is no lymphadenopathy. What is the most likely explanation for this patient’s symptoms?
A 52-year-old man comes to the physician because of right knee pain and swelling for 2 days. Four days ago, he tripped at home and landed on his knees. He reports an episode of diarrhea 3 weeks ago that resolved after 4 days without treatment. He has a history of hypertension and hypercholesterolemia, and was recently diagnosed with parathyroid disease. He drinks 1–2 ounces of whiskey daily and occasionally more on weekends. His brother has ankylosing spondylitis. Vital signs are within normal limits. Examination of the right leg shows an abrasion below the patella. There is swelling and tenderness of the right knee; range of motion is limited by pain. Arthrocentesis of the right knee joint yields 15 mL of cloudy fluid with a leukocyte count of 26,300/mm3 (91% segmented neutrophils). Microscopic examination of the synovial fluid under polarized light shows rhomboid-shaped, weakly positively birefringent crystals. Which of the following is the strongest predisposing factor for this patient's condition?
Practice by Chapter
Liver pathology (hepatitis, cirrhosis)
Practice Questions
Gallbladder and biliary tract disorders
Practice Questions
Pancreatic diseases
Practice Questions
Kidney diseases
Practice Questions
Male reproductive pathology
Practice Questions
Female reproductive pathology
Practice Questions
Breast pathology
Practice Questions
Endocrine pathology
Practice Questions
Bone and joint pathology
Practice Questions
Skeletal muscle diseases
Practice Questions
Peripheral nerve disorders
Practice Questions
Soft tissue tumors
Practice Questions
Head and neck pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app