
Systemic Pathology — MCQs

On this page
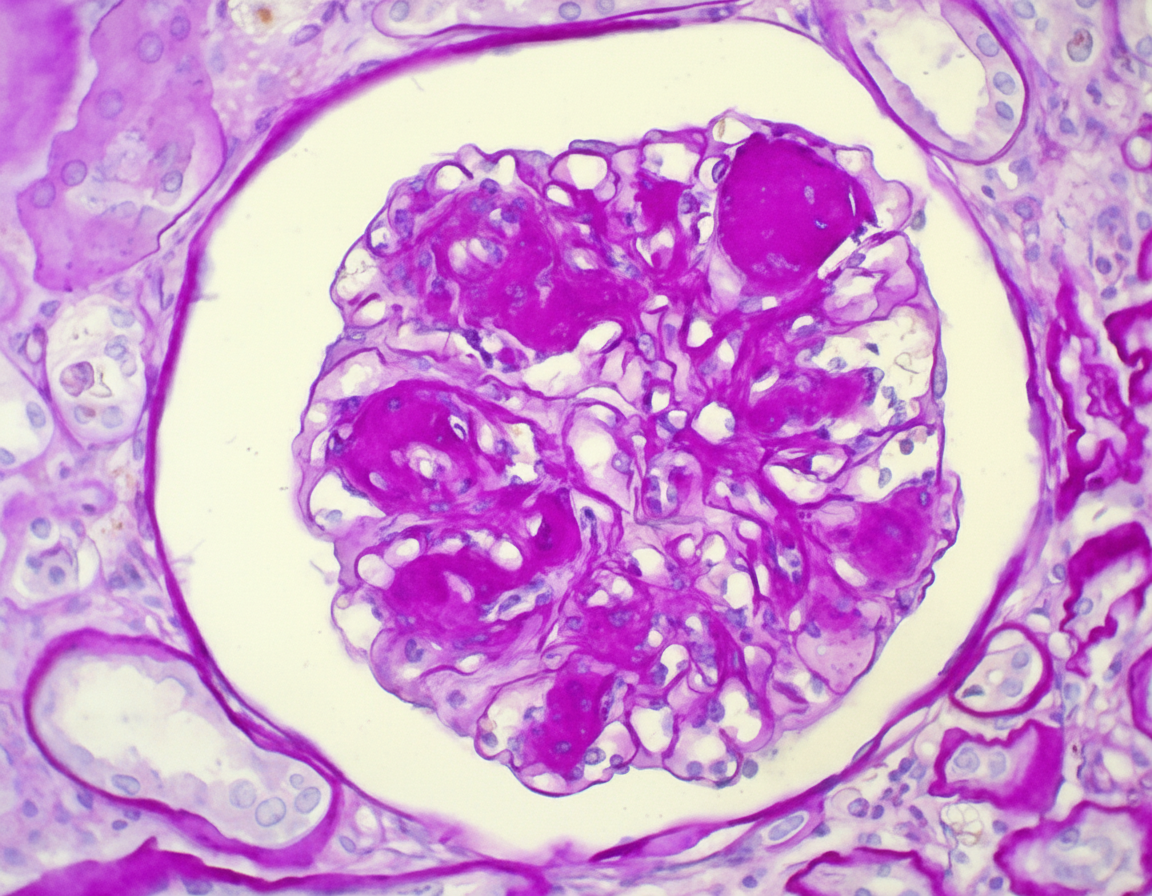
A 64-year-old man comes to the physician because of fatigue and decreased urinary frequency for 6 months. He has a 15-year history of type 2 diabetes mellitus and his most recent hemoglobin A1c was 9.2%. His pulse is 86/min and blood pressure is 150/90 mm Hg. Examination shows 1+ edema on bilateral ankles. His serum creatinine is 2 mg/dL and blood urea nitrogen is 28 mg/dL. Urinalysis shows proteinuria. A photomicrograph of a biopsy specimen from the patient's kidney is shown, revealing PAS-positive nodular mesangial sclerosis. Which of the following is the most likely explanation for the patient's biopsy findings?
A 12-year-old boy is brought to an outpatient clinic by his mother, who noticed that her son’s urine has been dark for the past 4 days. She initially attributed this to inadequate hydration, so she monitored her son’s fluid intake and encouraged him to drink more water. However, she noticed that the color of the urine kept getting darker until it began to resemble cola. The boy’s medical history is significant for a sore throat approx. 2 weeks ago, which resolved without medication or treatment. The boy has also been complaining of pain in his ankles, which he first noticed shortly after soccer practice 1 week ago. He has had no pain during urination or urethral discharge, however, and does not have any history of previous episodes of cola-colored urine or passage of blood in the urine. However, the boy has been experiencing intermittent episodes of abdominal pain for the past 3 days. The boy also has wheals on his torso, legs, and buttocks, which his mother attributes to seasonal allergies. Physical examination reveals an alert child who is not in obvious distress but who has a mild conjunctival pallor. Vital signs include: respiratory rate is 22/min, temperature is 36.7°C (98.0°F), and blood pressure is 130/90 mm Hg. Examination of the musculoskeletal system reveals multiple skin lesions (see image). Which of the following laboratory findings is most likely associated with this patient’s clinical presentation?

A 55-year-old male presents to his primary care physician complaining of right hip pain for the past eight months. He also reports progressive loss of hearing over the same time period. Radiographic imaging reveals multiple areas of expanded bony cortices and coarsened trabeculae in his right hip and skull. Laboratory analysis reveals an isolated elevation in alkaline phosphatase with normal levels of serum calcium and phosphate. Which of the following histologic findings is most likely to be seen if one of the lesions were biopsied?
A 57-year-old man presents to his primary care physician with a 2-month history of right upper and lower extremity weakness. He noticed the weakness when he started falling far more frequently while running errands. Since then, he has had increasing difficulty with walking and lifting objects. His past medical history is significant only for well-controlled hypertension, but he says that some members of his family have had musculoskeletal problems. His right upper extremity shows forearm atrophy and depressed reflexes while his right lower extremity is hypertonic with a positive Babinski sign. Which of the following is most likely associated with the cause of this patient's symptoms?
A 3-year-old girl is brought to her pediatrician because of a nosebleed that will not stop. Her parents say that she started having a nosebleed about 1 hour prior to presentation. Since then they have not been able to stop the bleeding. Her past medical history is remarkable for asthma, and she has a cousin who has been diagnosed with hemophilia. Physical exam reveals diffuse petechiae and purpura. A panel of bleeding tests are obtained with the following results: Bleeding time: 11 minutes Prothrombin time: 14 seconds Partial thromboplastin time: 32 seconds Platelet count: 195,000/mm^3 Peripheral blood smear shows normal cell morphology. Which of the following characteristics is most likely true about this patient?
An 8-year-old boy is brought to the physician by his parents because of fever for 3 days. During the period, he has had fatigue, severe burning with urination, and increased urination. The mother reports that his urine has red streaks and a “strange” odor. He has taken acetaminophen twice a day for the past two days with no improvement in his symptoms. He has had multiple ear infections in the past but has been healthy in the past year. His immunizations are up-to-date. He appears uncomfortable. His temperature is 39°C (102.2°F). Examination shows right-sided costovertebral angle tenderness. Laboratory studies show a leukocyte count of 16,000/cm3 and an erythrocyte sedimentation rate of 40 mm/hr. Urine dipstick shows leukocyte esterase and nitrites. Urinalysis shows: Blood 2+ Protein 2+ WBC 24/hpf RBC 50/hpf RBC casts none WBC casts numerous Granular casts none Urine cultures are sent to the laboratory. Damage to which of the following structures is the most likely cause of this patient's hematuria?
A 42-year-old woman comes to the physician because of a 10-month history of joint pain and stiffness in her wrists and fingers. The symptoms are worse in the morning and improve with activity. Physical examination shows swelling and warmth over the MCP and wrist joints in both hands. An x-ray of the hands is shown. Synovial biopsy from an affected joint would most likely show which of the following?

An 8-year-old boy is brought to the pediatrician because his mother is concerned about recent behavioral changes. His mother states that she has started to notice that he is slurring his speech and seems to be falling more than normal. On exam, the pediatrician observes the boy has pes cavus, hammer toes, and kyphoscoliosis. Based on these findings, the pediatrician is concerned the child has a trinucleotide repeat disease. Which of the following trinucleotide repeats is this child most likely to possess?
A 52-year-old man presents to the Emergency Department because of bilateral leg swelling and puffiness of both eyes in the morning. His symptoms started about 2 weeks ago. He denies smoking or alcohol use and his family history is noncontributory. Today, his vital signs include a temperature of 36.8°C (98.2°F), blood pressure of 162/87 mm Hg, and a pulse of 85/min. On physical examination, he is jaundiced and there is hepatosplenomegaly and 2+ lower extremity edema up to the mid-thigh. Laboratory results are shown: Anti-HCV reactive Serum albumin 3 g/dL Urine dipstick 3+ protein Urinalysis 10–15 red blood cells/high power field and red cell casts Which of the following is a feature of this patient’s condition?
A 22-year-old man comes to the physician because of a 2-week history of cough and decreased urination. The cough was initially nonproductive, but in the last few days he has coughed up small amounts of blood-tinged sputum with clots. He has not had any fevers, chills, or weight loss. He has smoked one pack of cigarettes daily for 5 years. Pulse is 115/min and blood pressure is 125/66 mm Hg. Physical examination shows dried blood around the lips. Serum studies show a creatinine of 2.9 mg/dL. Results of a serum antineutrophil cytoplasm antibody test are negative. A biopsy specimen of the kidney is most likely to show which of the following light microscopy findings?
Practice by Chapter
Liver pathology (hepatitis, cirrhosis)
Practice Questions
Gallbladder and biliary tract disorders
Practice Questions
Pancreatic diseases
Practice Questions
Kidney diseases
Practice Questions
Male reproductive pathology
Practice Questions
Female reproductive pathology
Practice Questions
Breast pathology
Practice Questions
Endocrine pathology
Practice Questions
Bone and joint pathology
Practice Questions
Skeletal muscle diseases
Practice Questions
Peripheral nerve disorders
Practice Questions
Soft tissue tumors
Practice Questions
Head and neck pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app