
Systemic Pathology — MCQs

On this page
A 58-year-old man comes to the physician because of a 3-month history of diffuse muscle pain, malaise, pain in both knees, recurrent episodes of abdominal and chest pain. He has also had a 5-kg (11-lb) weight loss over the past 4 months. Four years ago, he was diagnosed with chronic hepatitis B infection and was started on tenofovir. There are several ulcerations around the ankle and calves bilaterally. Perinuclear anti-neutrophil cytoplasmic antibodies are negative. Urinalysis shows proteinuria and hematuria. Muscle biopsy shows a transmural inflammation of the arterial wall with leukocytic infiltration and fibrinoid necrosis. Which of the following is the most likely diagnosis?
An 8-year-old boy is brought by his mother to his pediatrician because his urine is tea-colored and his face has appeared puffy for the past 2 days. He suffered a fever and sore throat several weeks ago that was treated with ibuprofen. The boy was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines and is meeting all developmental milestones. Today, his heart rate is 100/min, the respiratory rate is 22/min, the blood pressure is 130/80 mm Hg, and the temperature is 36.8°C (98.2°F). On physical exam the boy has mild periorbital swelling. A urine dipstick reveals 1+ proteinuria and urinalysis reveals 10–15 red cells/high power field and dysmorphic red cells. The pediatrician is concerned with the child’s hypertension, facial edema, and abnormal urine analysis results. Which of the following best represents the mechanism of this patient’s condition?
A 39-year-old man presents to his primary care physician with new onset lower extremity edema, fatigue, and hematuria. His symptoms began approximately 2 weeks prior to presentation and have progressively worsened. Medical history is significant for opioid-use disorder with heroin treated with methadone. He is in a monogamous relationship with a female partner of 4 years and does not use condoms. He denies cigarette smoking, alcohol use, and last used heroin approximately 1 month ago. His temperature is 99°F (37.2°C), blood pressure is 152/98 mmHg, pulse is 83/min, and respirations are 17/min. On physical exam, there is conjunctival pallor, scleral icterus, a 14 cm liver span, acrocyanosis, and lower extremity 2+ pitting edema. Urinalysis demonstrates proteinuria and dysmorphic red blood cells. Laboratory testing reveals a mildly decreased C3 and decreased C4 serum concentration. Which of the following will most likely be present on renal biopsy in this patient?
A 73-year-old man dies 4 months after being diagnosed with advanced adenocarcinoma of the colon. Examination of the heart at autopsy shows vegetations lining the mitral valve margins. The vegetations are loosely attached and can be easily scraped off. Microscopic examination shows the vegetations to be composed of interwoven fibrin strands with mononuclear cells. The mitral valve endothelium is intact. Which of the following is the most likely underlying cause of these autopsy findings?
A 36-year-old woman comes to the physician for evaluation of unintentional weight gain of 5.5 kg (12.2 lb) and irregular menstrual cycles over the past 2 months. She does not take any medications. Her blood pressure is 155/85 mm Hg. Physical examination shows central obesity, hyperpigmentation of the palmar creases, and violaceous scarring of the abdomen. Early morning serum cortisol levels are elevated and serum adrenocorticotropic hormone (ACTH) is within the reference range after a low-dose dexamethasone suppression test. A high-dose dexamethasone suppression test shows suppression of ACTH. Further evaluation is most likely to show which of the following findings?
A 3-year-old African-American boy presents with a rapid onset of severe abdominal pain. He has a palpably enlarged mass in the left upper quadrant of his abdomen. Complete blood count is notable for a hemoglobin of 7.2 g/dL. Serum haptoglobin level returns normal. Serum unconjugated bilirubin is elevated. The corrected reticulocyte count is elevated. Which of the following is the most likely explanation for the findings above?
A 62-year-old woman is seen in the hospital for neutropenic fever. She was admitted 1 week ago for newly diagnosed acute myeloid leukemia. Due to her chemotherapy, she became pancytopenic. Last night, during a packed red blood cell transfusion, she became febrile to 102.6°F (39.3°C), her blood pressure was 92/55, pulse was 112/min, respirations were 16/min, and oxygen saturation was 94% on room air. The transfusion was stopped, intravenous fluids were started, and blood cultures were drawn. The patient also complained of chest pain and shortness of breath. A chest radiograph was obtained and was normal. This morning, she reports "dark urine" but denies dysuria or abnormal vaginal discharge. Her prophylactic antimicrobials started at the time of her chemotherapy include acyclovir, levofloxacin, and fluconazole. The patient's temperature this morning is 98.7°F (37.1°C), blood pressure is 110/72 mmHg, pulse is 88/min, and respirations are 17/min with an oxygen saturation of 95% on room air. On physical examination, she has 1+ pitting peripheral edema of bilateral lower extremities to the mid-shin. Her jugular venous pressure is 6 cm. Her labs show neutropenia, normocytic anemia, thrombocytopenia, elevated lactate dehydrogenase, elevated total bilirubin, and decreased haptoglobin. Coagulation studies show an increase in bleeding time with normal D-dimer levels. Which of the following is the most likely cause of the patient's symptoms?
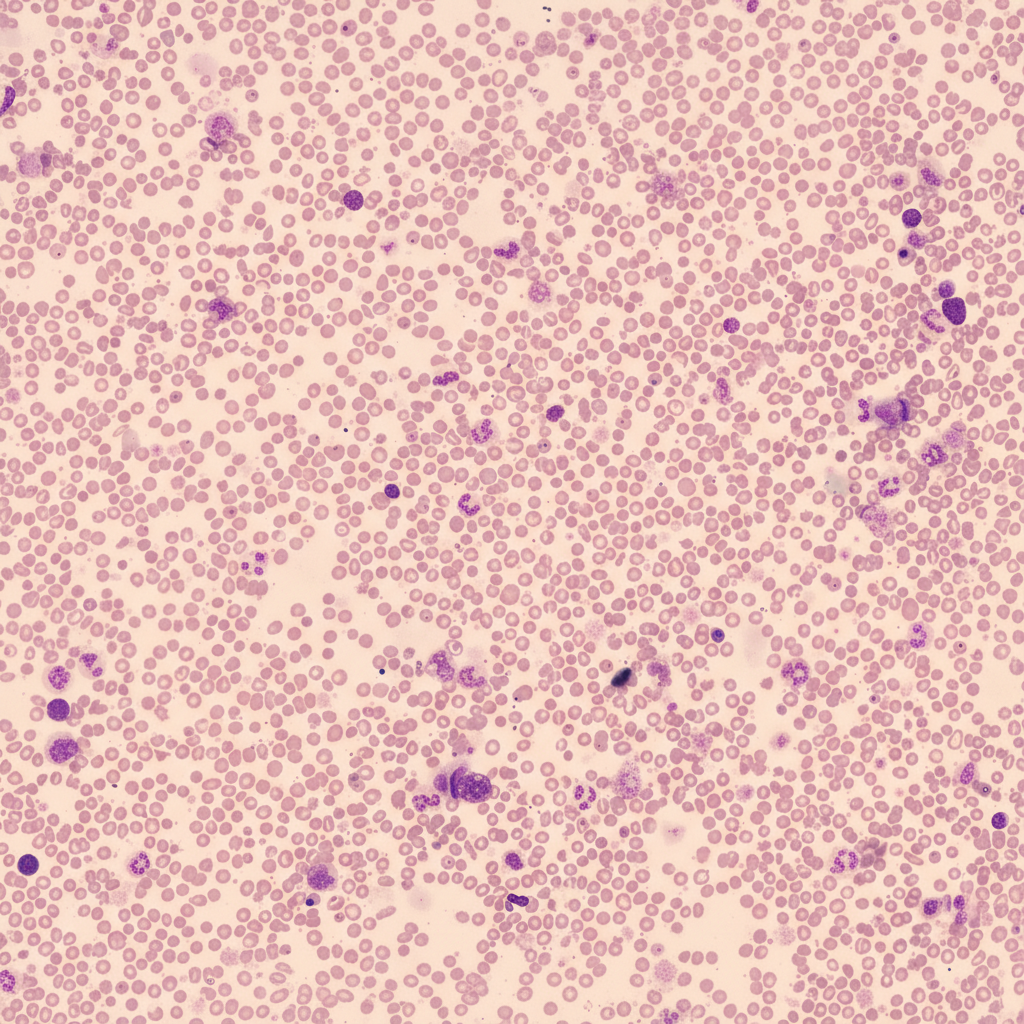
A 51-year-old man presents to his primary care physician with 3 months of increasing fatigue. He says that he has been feeling short of breath while walking to his office from the parking lot and is no longer able to participate in recreational activities that he enjoys such as hiking. His wife also comments that he has been looking very pale even though they spend a lot of time outdoors. His past medical history is significant for acute kidney injury after losing blood during a car accident as well as alcoholic hepatitis. Physical exam reveals conjunctival pallor, and a peripheral blood smear is obtained with the finding demonstrate in figure A. Which of the following is associated with the most likely cause of this patient's symptoms?
A 70-year-old woman comes to the physician because of a 4-month history of fatigue, worsening swelling of her ankles, and a 5-kg (11-lb) weight gain. Neurologic examination shows diminished two-point discrimination in her fingers. Laboratory studies show a hemoglobin A1c concentration of 9.2% and a creatinine concentration of 1.3 mg/dL. Urine dipstick shows heavy proteinuria. A biopsy specimen of this patient's kidney is most likely to show which of the following?
A 21-year-old woman comes to the physician because of a 1-week history of shortness of breath and dry cough. Eight weeks ago, she received a lung transplant from an unrelated donor. Current medications include prednisone, cyclosporine, and azathioprine. Her temperature is 37.8°C (100.1°F). Physical examination is unremarkable other than a well-healed surgical scar. Pulmonary function tests show a decline in FEV1 and FVC compared to values from several weeks ago. Histological examination of a lung biopsy specimen shows perivascular and interstitial lymphocytic infiltrates with bronchiolar inflammation. This patient's condition is most likely caused by T cell sensitization against which of the following?
Practice by Chapter
Liver pathology (hepatitis, cirrhosis)
Practice Questions
Gallbladder and biliary tract disorders
Practice Questions
Pancreatic diseases
Practice Questions
Kidney diseases
Practice Questions
Male reproductive pathology
Practice Questions
Female reproductive pathology
Practice Questions
Breast pathology
Practice Questions
Endocrine pathology
Practice Questions
Bone and joint pathology
Practice Questions
Skeletal muscle diseases
Practice Questions
Peripheral nerve disorders
Practice Questions
Soft tissue tumors
Practice Questions
Head and neck pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app