
Systemic Pathology — MCQs

On this page
A 32-year-old woman presents to the office with complaints of frothy urine and swelling in her body that started 6 days ago. She says that she first noticed the swelling in her face that gradually involved other parts of her body. On further questioning, she gives a history of rheumatoid arthritis for 2 years. She is taking Penicillamine and Methotrexate for the past 6 months. Vitals include: blood pressure 122/89 mm Hg, pulse rate 55/min, temperature 36.7°C (98.0°F), and a respiratory rate 14/min. On examination, there is generalized pitting edema along with some subcutaneous nodules on the dorsal aspect of the forearm. Urinalysis pH 6.6 Color light yellow RBC none WBC 1–2/HPF Protein 4+ Cast fat globules Glucose absent Crystal none Ketone absent Nitrite absent 24 hours urine protein excretion 4.8 g Basic metabolic panel Sodium 141 mEq/L Potassium 5.1 mEq/L Chloride 101 mEq/L Bicarbonate 22 mEq/L Albumin 3.2 mg/dL Urea nitrogen 17 mg/dL Creatinine 1.3 mg/dL Uric Acid 6.8 mg/ dL Calcium 8.9 mg/ dL Glucose 111 mg/dL A renal biopsy is ordered which shows diffuse capillary and glomerular basement membrane thickening. Which of the following is the most likely cause for her impaired renal function?
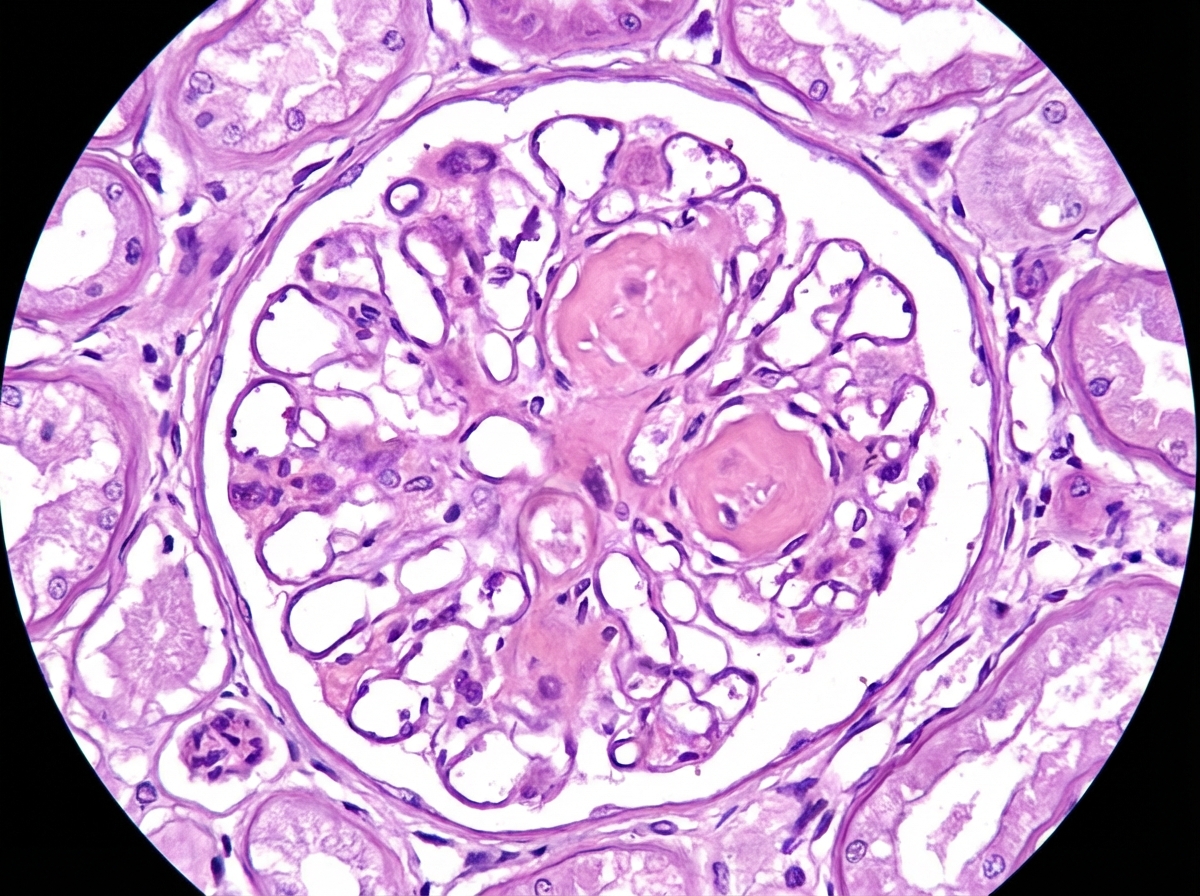
A 62-year-old man comes to the physician because of fatigue and decreased urine output for 2 weeks. He has not been to the physician for many years and takes no medications. Serum studies show a urea nitrogen concentration of 42 mg/dL and a creatinine concentration of 2.3 mg/dL. HbA1c is 10.2%. Urinalysis shows heavy proteinuria. A photomicrograph of a section of a kidney biopsy specimen is shown; the biopsy stains PAS-positive and Congo red-negative. Which of the following is the most likely underlying cause of this patient's symptoms?
An 80-year-old woman died due to the respiratory complications of lung cancer. She had been a heavy smoker, and battled COPD and adenocarcinoma of the lungs for the last 20 years. The autopsy also revealed a pathological finding in the mitral valve. Which of the following was most likely seen?
A 30-year-old man presents to the emergency department with complaints of red, pinkish urine in the morning. He adds that he has been feeling some abdominal pain. The patient is not taking any medication, and his laboratory test results are as follows: Hb 11.0 g/dL RBC 3.7 x 1012/L WBC 4,000/mm3 PLT 100,000/mm3 Reticulocytes 17% of red cells Coombs test Negative Blood smear Polychromasia Which statement is true about this patient’s condition?
A 49-year-old female with a long history of poorly controlled diabetes mellitus visits her primary care physician with 2+ non-pitting edema in her legs. The patient has a serum creatinine of 2.9 mg/dL and a blood urea nitrogen of 61 mg/dL. A 24-hour urine collection reveals 8.5 grams of protein. A renal biopsy is obtained. Which of the following histologic findings is most likely to be seen upon tissue analysis:
A 26-year-old woman presents with episodes of intermittent fever, arthralgias, constant fatigue, weight loss, and plaque-like rash on sun-exposed areas, which have been gradually increasing over the last 6 months. On presentation, her vital signs include: blood pressure is 110/80 mm Hg, heart rate is 87/min, respiratory rate is 14/min, and temperature is 37.5°C (99.5°F). Physical examination reveals an erythematous scaling rash on the patient’s face distributed in a ‘butterfly-like’ fashion, erythematous keratinized patches on the sun-exposed areas, and mild lower leg edema. During the workup, the patient is found to be positive for anti-Sm (anti-Smith) antibodies. Which process is altered in this patient?
A 47-year-old woman presents for a routine wellness checkup. She complains of general fatigue and lethargy for the past 6 months. She does not have a significant past medical history and is currently not taking any medications. The patient reports that she drinks “socially” approx. 6 nights a week. She says she also enjoys a “nightcap,” which is 1–2 glasses of wine before bed every night. She denies any history of drug use or smoking. The patient is afebrile, and her vital signs are within normal limits. A physical examination reveals pallor of the mucous membranes. Her laboratory findings are significant for a mean corpuscular volume of 72 fL, leukocyte count of 5,300/mL, hemoglobin of 11.0 g/dL, and platelet count of 420,000/mL. Which of the following is the most likely cause of this patient’s thrombocytosis?
A 25-year-old woman comes to the physician because of recurrent episodes of reddish discoloration of her urine. She also has a 3-month history of intermittent abdominal pain, yellowish discoloration of the skin and eyes, and fatigue. Physical examination shows pallor and scleral icterus. The spleen is not palpable. Her hemoglobin concentration is 7.8 g/dL, leukocyte count is 2,000/mm3, and platelet count is 80,000/mm3. Serum LDH and unconjugated bilirubin concentrations are elevated. Addition of a serum containing anti-human globulins to a blood sample shows no agglutination. A urine dipstick shows blood; urinalysis shows no RBCs. A CT scan of the abdomen shows a thrombus in a distal branch of the superior mesenteric vein. Which of the following is the most likely cause of this patient's condition?
A 15-year-old girl presents with menorrhagia for the last 4 months. The patient’s mother says that she just started getting her period 4 months ago, which have been heavy and prolonged. The patient does recall getting a tooth extracted 3 years ago that was complicated by persistent bleeding afterward. She has no other significant past medical history and takes no current medications. Her vital signs include: blood pressure 118/76 mm Hg, respirations 17/min, pulse 64/min, temperature 36.7°C (98.0°F). Physical examination is unremarkable. Which of the following laboratory tests is most likely to be of the greatest diagnostic value in the workup of this patient?
A 22-year-old man comes to the physician because of several episodes of painless bloody urine over the past 6 months. The episodes are not related to physical activity. He has had frequent nosebleeds since early childhood and an episode of heavy bleeding after a tooth extraction one year ago. He smokes one pack of cigarettes daily. He drinks 1 to 2 beers on social occasions. He appears pale. His vital signs are within normal limits. Physical examination shows several small hematomas in different stages of healing over his arms and legs. Examination of the extremities shows decreased passive range of motion with crepitus in both ankles. His abdomen is soft and nontender. Laboratory studies show: Hemoglobin 9.5 mg/dL Leukocyte count 5000/mm3 Platelet count 240,000/mm3 Bleeding time 5 minutes Prothrombin time 14 seconds Partial thromboplastin time 68 seconds Urine RBC 30–40/hpf RBC casts negative WBC none Protein negative An x-ray of the pelvis shows no abnormalities. Further evaluation of this patient is most likely to show which of the following findings?
Practice by Chapter
Liver pathology (hepatitis, cirrhosis)
Practice Questions
Gallbladder and biliary tract disorders
Practice Questions
Pancreatic diseases
Practice Questions
Kidney diseases
Practice Questions
Male reproductive pathology
Practice Questions
Female reproductive pathology
Practice Questions
Breast pathology
Practice Questions
Endocrine pathology
Practice Questions
Bone and joint pathology
Practice Questions
Skeletal muscle diseases
Practice Questions
Peripheral nerve disorders
Practice Questions
Soft tissue tumors
Practice Questions
Head and neck pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app