
Systemic Pathology — MCQs

On this page
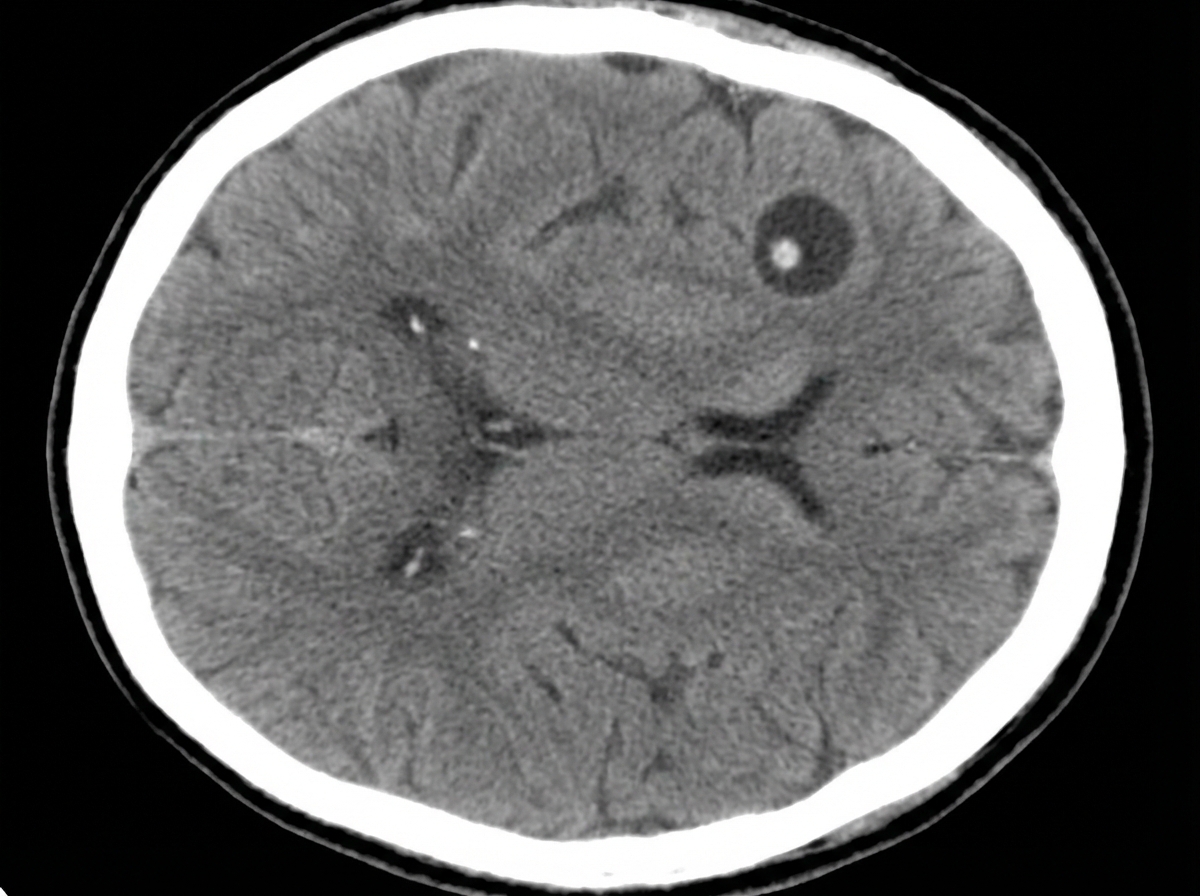
A 53-year-old woman with hypertension is brought to the emergency department 30 minutes after having a generalized, tonic-clonic seizure. She has had recurrent headaches and dizziness in the last 3 months. One year ago, she had diarrhea after a trip to Ecuador that resolved without treatment. She has not received any medical care in the last five years. She has smoked 1 pack of cigarettes daily for 20 years. Her temperature is 36°C (96.8°F) and blood pressure is 159/77mm Hg. Physical examination shows dysarthria and hyperreflexia. She is confused and oriented only to name and place. Four brain lesions are found in a CT scan of the brain; one of the lesions is shown. Which of the following is most likely to have prevented this patient's condition?
A 16-year-old boy is brought to the pediatrician by his mother because she is concerned about the “spots” on his abdomen and back. The patient’s mother reports that there are several “light spots” on the patient’s trunk that have been slowly increasing in number. The lesions are not painful nor pruritic. The patient’s mother is worried because her nephew had vitiligo. The patient reports that he feels “fine,” but reports occasional headaches and increasing difficulty with seeing the board at school. In addition to the patient’s cousin having vitiligo, the patient’s paternal grandfather and uncle have bilateral deafness, and his mother has systemic lupus erythematous. On physical examination, there are multiple, discrete, 2-3 cm hypopigmented macules on the chest, abdomen, back, and posterior shoulders. Which of the following head and neck computed tomography findings is the patient most likely to develop?
A 72-year-old African American man presents with progressive fatigue, difficulty breathing on exertion, and lower extremity swelling for 3 months. The patient was seen at the emergency department 2 times before. The first time was because of back pain, and the second was because of fever and cough. He took medications at the emergency room, but he refused to do further tests recommended to him. He does not smoke or drink alcohol. His family history is irrelevant. His vital signs include a blood pressure of 110/80 mm Hg, temperature of 37.2°C (98.9°F), and regular radial pulse of 90/min. On physical examination, the patient looks pale, and his tongue is enlarged. Jugular veins become distended on inspiration. Pitting ankle edema is present on both sides. Bilateral basal crackles are audible on the chest auscultation. Hepatomegaly is present on abdominal palpation. Chest X-ray shows osteolytic lesions of the ribs. ECG shows low voltage waves and echocardiogram shows a speckled appearance of the myocardium with diastolic dysfunction and normal appearance of the pericardium. Which of the following best describes the mechanism of this patient’s illness?
A 56-year-old African-American man comes to the physician for intermittent episodes of dark urine and mild flank pain. The patient has had 3 episodes of frank reddish discoloration of his urine within 1 month. He has chronic headaches and back pain for which he has been taking aspirin and ibuprofen daily for 1 year. The patient has sickle cell trait. He has smoked a pack of cigarettes daily for 10 years. He appears well. His temperature is 37.4°C (99.3°F). His pulse is 66/min, and his blood pressure is 150/90 mm Hg. Physical exam shows mild, bilateral flank tenderness. Laboratory analysis shows a serum creatinine concentration of 2.4 mg/dL. Urine studies are shown below. Urine Blood 3+ Protein 2+ RBC > 10/hpf WBC 3/hpf Which of the following is the most likely underlying cause of this patient's hematuria?
A 67-year-old male presents with left hip pain. Examination reveals mild effusions in both knees, with crepitus in both patellofemoral joints. He states his hearing has worsened recently and that he feels like his hats don't fit anymore. Bone scan reveals diffuse uptake in the calvarium, right proximal femur, and left ilium. Which of the following laboratory abnormalities would be expected in this patient?
A 23-year-old woman presents to the emergency department with a 3-day history of fever and headache. She says that the symptoms started suddenly after she woke up 3 days ago, though she has been feeling increasingly fatigued over the last 5 months. On presentation, her temperature is 102°F (38.9°C), blood pressure is 117/74 mmHg, pulse is 106/min, and respirations are 14/min. Physical exam reveals diffuse petechiae and conjunctival pallor and selected laboratory results are shown as follows: Bleeding time: 11 minutes Platelet count: 68,000/mm^3 Lactate dehydrogenase: 105 U/L Which of the following would also most likely be true for this patient?
A previously healthy 6-year-old girl is brought to the physician by her parents because of slowed growth and fatigue. Over the past year, she went from average height for her age group to the shortest in her class. She has also been having more problems concentrating in class and is less interested in playing. She has not had any change in appetite or diet. She is at the 10th percentile for height and the 90th percentile for weight. Vital signs are within normal limits. There is a nontender mass palpated on the anterior cervical examination. Serum laboratory studies show thyroid-stimulating hormone level of 6.7 μU/mL. Further evaluation is most likely to show which of the following findings?
A 19-year-old woman presents to the primary care clinic to establish care. She has no acute complaints or concerns. Upon further questioning, she shares that she gets frequent nosebleeds and often bleeds from her gums a little after brushing her teeth. She also typically has relatively heavy menstrual periods, soaking eight tampons per day. She has not had any serious bleeding events, and she has never had a blood transfusion. Physical exam is unremarkable. A complete blood count shows mild anemia with a normal platelet count. Which of the following is the next best step in the management of this patient?
A 61-year-old construction worker comes to the physician because of a 3-month history of progressively worsening cough and shortness of breath. He has had a 7.5-kg (16.5-lb) weight loss during this period. He smokes occasionally and does not drink alcohol. Physical examination shows clubbing of the fingers. End-inspiratory crackles are heard in both lower lung fields. X-ray of the chest shows bilateral reticulonodular densities with interstitial fibrosis. Histologic examination of a lung biopsy specimen shows noncaseating granulomas in the interstitium. Which of the following is the most likely underlying mechanism of this patient's condition?
A 67-year-old male presents to his primary care physician complaining of left hip pain for the past six months. He denies any trauma or recent falls. He is accompanied by his wife who reports that he has experienced progressive hearing loss over the same time period. The patient has also noticed that he is no longer able to fit into his favorite hat even though it previously fit well. A radiograph of the patient’s pelvis is shown. Which of the following laboratory abnormalities is most likely to be found in this patient?

Practice by Chapter
Liver pathology (hepatitis, cirrhosis)
Practice Questions
Gallbladder and biliary tract disorders
Practice Questions
Pancreatic diseases
Practice Questions
Kidney diseases
Practice Questions
Male reproductive pathology
Practice Questions
Female reproductive pathology
Practice Questions
Breast pathology
Practice Questions
Endocrine pathology
Practice Questions
Bone and joint pathology
Practice Questions
Skeletal muscle diseases
Practice Questions
Peripheral nerve disorders
Practice Questions
Soft tissue tumors
Practice Questions
Head and neck pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app