
Systemic Pathology — MCQs

On this page
A 34-year-old woman with beta-thalassemia major is brought to the physician because of a 2-month history of fatigue, darkening of her skin, and pain in her ankle joints. She has also had increased thirst and frequent urination for 2 weeks. She receives approximately 5 blood transfusions every year; her last transfusion was 3 months ago. Physical examination shows hyperpigmented skin, scleral icterus, pale mucous membranes, and a liver span of 17 cm. Which of the following serum findings is most likely in this patient?
A 3-year-old boy is brought to the physician for evaluation of pallor and increasing lethargy for 3 days. Six days ago, he experienced abdominal pain, vomiting, and bloody diarrhea that have since resolved. The family returned from a road trip to Mexico 4-weeks ago. His temperature is 38.8°C (101.8°F), pulse is 128/min, respirations are 30/min, and blood pressure is 96/60 mm Hg. Examination shows pale conjunctivae and scleral icterus. The abdomen is soft, nontender, and nondistended. Bowel sounds are hyperactive. Laboratory studies show: Hemoglobin 7.8 g/dL Mean corpuscular volume 92 μm3 Leukocyte count 18,500/mm3 Platelet count 45,000/mm3 Prothrombin time 12 sec Partial thromboplastin time 34 sec Serum Urea nitrogen 32 mg/dL Creatinine 1.8 mg/dL Bilirubin Total 2.0 mg/dL Direct 0.1 mg/dL Lactate dehydrogenase 1685 U/L A peripheral blood smear shows schistocytes. Which of the following is the most likely mechanism of this patient's presentation?
A 34-year-old woman comes to the physician because of recent fatigue and weakness that is exacerbated by cross-country skiing. Four weeks ago, she was diagnosed with pneumonia; sputum cultures on Eaton agar showed organisms that lacked a cell wall. Physical examination shows conjunctival pallor and cyanosis of the fingertips. Both lungs are clear to auscultation. Which of the following findings is most likely to confirm the diagnosis?
A 30-year-old Caucasian male presents with hemoptysis and uremia. Blood tests show the presence of anti-basement membrane antibodies specific for collagen located in glomerular and pulmonary basement membranes. The patient undergoes plasmapheresis to help reduce the amount of anti-basement membrane antibodies. Which of the following diseases is of the same hypersensitivity category as this disease?
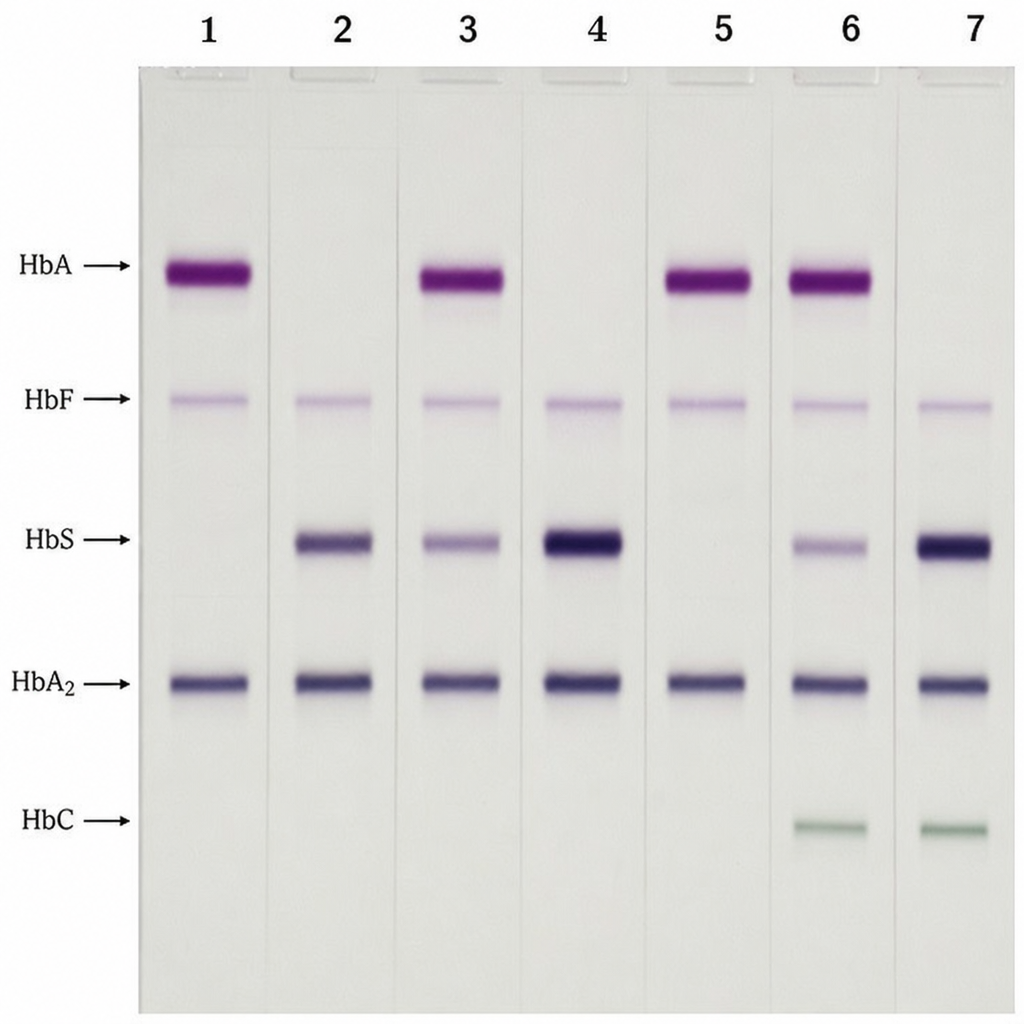
A 7-year-old girl with a history of painful crises and impaired growth presents for evaluation of sickle cell disease. You perform hemoglobin gel electrophoresis, and diagnose her with homozygous sickle cell disease. Which of the gel electrophoresis lanes in the image is hers?
A 62-year-old man presents to the emergency department with a 2-day history of fatigue, exertional dyspnea, and the sensation of his heartbeat roaring in the ears. He informs you that he recently had an acute upper respiratory infection. He is a retired car salesman, and he informs you that he and his partner enjoy traveling to the tropics. His medical history is significant for gout, hypertension, hypercholesterolemia, diabetes mellitus type II, and multiple basal cell carcinomas on his face and neck. He currently smokes 1 pack of cigarettes per day, drinks a 6-pack of beer per day, and denies any illicit drug use. His vital signs include: temperature 36.7°C (98.0°F), blood pressure 126/74 mm Hg, heart rate 111/min, and respiratory rate 23/min. On physical examination, his pulses are bounding, his complexion is pale, and scleral icterus is apparent. The spleen is moderately enlarged. Oxygen saturation was initially 81% on room air, with a new oxygen requirement of 8 L by face mask. Laboratory analysis results show a hemoglobin level of 7.1 g/dL and elevated total bilirubin. Of the following options, which laboratory test can help to make the diagnosis?
A 63-year-old woman is brought to the physician by her husband for the evaluation of progressive memory loss for the past 5 months. During the last 2 weeks, she has also had problems getting dressed and finding her way back home from the grocery store. She has had several episodes of jerky, repetitive, twitching movements that resolved spontaneously. She used to work as a teacher but quit her job due to her memory loss. The patient has hypertension. There is no family history of serious illness. Her only medication is hydrochlorothiazide. Her temperature is 37°C (98.6°F), pulse is 65/min, and blood pressure is 125/80 mmHg. She is oriented only to person and place. She follows commands and speaks fluently, but sometimes cannot recall objects. She is unable to read and seems to have difficulty recognizing objects. Cranial nerves II-XII are intact. Examination shows full muscle strength. Deep tendon reflexes are 2+ bilaterally. Babinski sign is absent. Sensation to pinprick and light touch is normal. Which of the following is the most likely underlying cause of this patient's symptoms?
A 21-year-old woman with a history of acute lymphoblastic leukemia comes to the physician because she has not had a menstrual period for 12 months. Menarche occurred at the age of 11 years, and menses occurred at regular 28-day intervals until they became irregular 1 year ago. Physical examination shows normal female genitalia and bimanual examination shows a normal-sized uterus. Laboratory studies show markedly elevated FSH levels consistent with premature ovarian failure. Fluorescence in situ hybridization studies show a 46,XY karyotype in the peripheral blood cells. Which of the following is the most likely explanation for the male karyotype found on chromosomal analysis?
A 1-year-old boy presents to the physician with a fever and a persistent cough for the past 5 days. His parents noted that since birth, he has had a history of recurrent skin infections, ear infections, and episodes of pneumonia with organisms including Staphylococcus aureus, Pseudomonas, and Candida. Physical exam is notable for prominent facial scars in the periorbital and nasal regions, which his parents explain are a result of healed abscesses from previous skin infections. A sputum sample is obtained from the patient and the culture grows Aspergillus. Which of the following diagnostic test findings would confirm the patient’s underlying genetic disease?
A 35-year-old woman comes to the physician for the evaluation of fatigue and dizziness for the past 2 months. During this period, she has also had mild upper abdominal pain that is not related to food intake. She has no personal or family history of serious illness. She immigrated to the United States from Italy 10 years ago. Menses occur at regular 28-day intervals with moderate flow. She does not smoke or drink alcohol. She takes no medications. Her vital signs are within normal limits. The spleen is palpated 2 cm below the left costal margin. There is no scleral icterus. Neurologic examination shows no abnormalities. Laboratory studies show: Hemoglobin 11.2 g/dL Mean corpuscular volume 62 μm3 Leukocyte count 7,000/mm3 Platelet count 260,000/mm3 A peripheral blood smear shows target cells. The patient is started on iron supplementation. Three weeks later, her laboratory studies are unchanged. Which of the following is the most likely underlying cause of this patient’s condition?
Practice by Chapter
Liver pathology (hepatitis, cirrhosis)
Practice Questions
Gallbladder and biliary tract disorders
Practice Questions
Pancreatic diseases
Practice Questions
Kidney diseases
Practice Questions
Male reproductive pathology
Practice Questions
Female reproductive pathology
Practice Questions
Breast pathology
Practice Questions
Endocrine pathology
Practice Questions
Bone and joint pathology
Practice Questions
Skeletal muscle diseases
Practice Questions
Peripheral nerve disorders
Practice Questions
Soft tissue tumors
Practice Questions
Head and neck pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app