
Systemic Pathology — MCQs

On this page
A 59-year-old woman comes to the physician because of upper extremity weakness and fatigue for the past 4 months. She has had difficulty combing her hair and lifting objects. She has also had difficulty rising from her bed in the mornings for 2 months. Over the past month, she started using over-the-counter mouth rinses for dry mouth. She has smoked 1 pack of cigarettes daily for 40 years. Examination shows decreased deep tendon reflexes. Repetitive muscle tapping shows increased reflex activity. There are no fasciculations or muscle atrophy. A low-dose CT scan of the chest shows a 3-cm mass with heterogeneous calcifications in the center of the right lung. Which of the following is the most likely underlying mechanism responsible for this patient’s current symptoms?
A 38-year-old woman comes to the physician because of a 1-month history of fatigue and pruritus. Examination of the abdomen shows an enlarged, nontender liver. Serum studies show an alkaline phosphatase level of 140 U/L, aspartate aminotransferase activity of 18 U/L, and alanine aminotransferase activity of 19 U/L. Serum antimitochondrial antibody titers are elevated. A biopsy specimen of this patient's liver is most likely to show which of the following findings?
A 42-year-old male presents to his primary care physician with complaints of fatigue and occasionally darkened urine over the past 3 months. Upon further questioning, the patient reveals that he has regularly had dark, 'cola-colored' urine when he has urinated at night or early in the morning. However, when he urinates during the day, it appears a much lighter yellow color. Laboratory work-up is initiated and is significant for a hemoglobin of 10.1 g/dL, elevated LDH, platelet count of 101,000/uL, and leukopenia. Urinalysis, taken from an early morning void, reveals brown, tea-colored urine with hemoglobinuria and elevated levels of hemosiderin. Which of the following is responsible for this patient's presentation?
A 39-year-old man presents to the emergency room for epistaxis. He reports having frequent nosebleeds over the past 48 hours. He also reports a constant pounding headache over the same timeframe. He is accompanied by his wife who reports that he has seemed "off" lately, frequently forgetting recent events and names of his friends. His past medical history is notable for hypertension and rheumatoid arthritis. He takes lisinopril and methotrexate. He has a 10 pack-year smoking history and drinks 2-3 beers per day. His temperature is 101.1°F (38.4°C), blood pressure is 145/90 mmHg, pulse is 110/min, and respirations are 18/min. On exam, he appears pale, diaphoretic, and has mild scleral icterus. His spleen is palpable but non-tender. Laboratory analysis is shown below: Hemoglobin: 8.9 g/dL Hematocrit: 26% Leukocyte count: 4,900/mm^3 with normal differential Platelet count: 25,000/mm^3 Prothrombin time: 14 seconds Partial thromboplastin time (activated): 27 seconds International normalized ratio: 1.1 Bleeding time: 9 minutes This patient has a condition that is caused by a defect in which of the following processes?
A 33-year-old woman is brought to the emergency department after she was involved in a high-speed motor vehicle collision. She reports severe pelvic pain. Her pulse is 124/min and blood pressure is 80/56 mm Hg. Physical examination shows instability of the pelvic ring. As part of the initial emergency treatment, she receives packed red blood cell transfusions. Suddenly, the patient starts bleeding from peripheral venous catheter insertion sites. Laboratory studies show decreased platelets, prolonged prothrombin time and partial thromboplastin time, and elevated D-dimer. A peripheral blood smear of this patient is most likely to show which of the following findings?
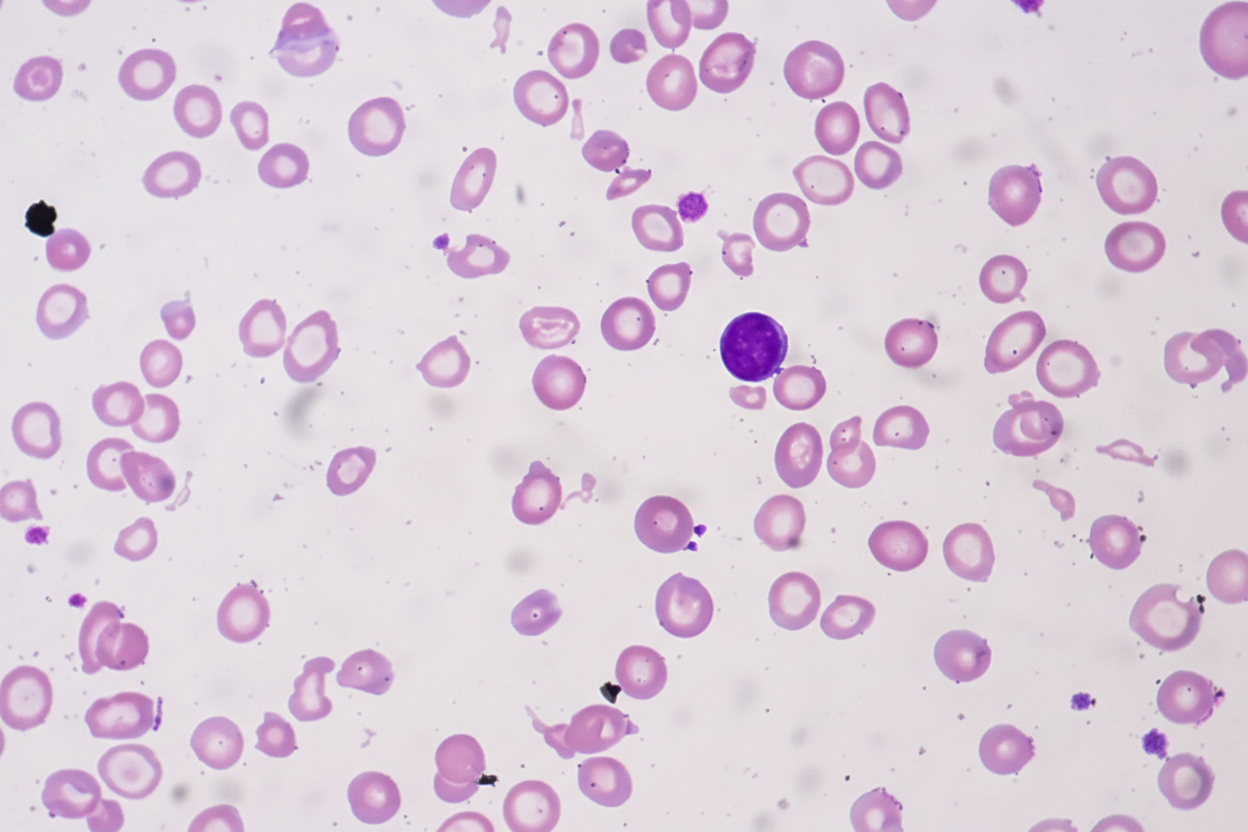
A 25-year-old African-American woman visits the doctor's office complaining of fatigue for a couple of months. She says that she feels exhausted by the end of the day. She works as a dental assistant and is on her feet most of the time. However, she eats well and also tries to walk for 30 minutes every morning. She also says that she sometimes feels breathless and has to gasp for air, especially when she is walking or jogging. Her past medical history is insignificant, except for occasional bouts of cold during the winters. Her physical exam findings are within normal limits except for moderate conjunctival pallor. Complete blood count results and iron profile are as follows: Hemoglobin 9 g/dL Hematocrit 28.5% RBC count 5.85 x 106/mm3 WBC count 5,500/mm3 Platelet count 212,000/mm3 MCV 48.7 fl MCH 15.4 pg/cell MCHC 31.6 g/dL RDW 11.7% Hb/cell Serum iron 170 mcg/dL Total iron-binding capacity (TIBC) 458 mcg/dL Transferrin saturation 37% A peripheral blood smear is given. When questioned about her family history of anemia, she says that all she remembers is her dad was never allowed to donate blood as he was anemic. Which of the following most likely explains her cell counts and blood smear results?
A 52-year-old man is diagnosed with chronic renal failure. He is on hemodialysis. The physicians have advised him that he needs a renal transplant. The human leukocyte antigen (HLA) genotype is A7/A5, B2/B9, and C8/C3. For each locus, the maternal allele is listed 1st and the paternal allele is listed 2nd. There are several potential donors available for the renal graft. Which of the following donors would be the closest match?
A 40-year-old male with a history of chronic alcoholism recently received a liver transplant. Two weeks following the transplant, the patient presents with a skin rash and frequent episodes of bloody diarrhea. A colonoscopy is performed and biopsy reveals apoptosis of colonic epithelial cells. What is most likely mediating these symptoms?
A 16-year-old presents to the primary care physician because he has noticed an increase in the size of his breast tissue over the past 3 years. He states that he is significantly taller than his entire class at school although he feels increasingly weak and uncoordinated. He performs at the bottom of his grade level academically. On physical exam the patient has marked gynecomastia with small firm testes. The physician decides to perform a karyotype on the patient. What is the most likely outcome of this test?
A 35-year-old African American man presents with fever, abdominal pain, and severe weakness since yesterday. On physical examination, the patient is jaundiced and shows a generalized pallor. Past medical history is significant for recently receiving anti-malaria prophylaxis before visiting Nigeria. Laboratory tests show decreased glucose-6-phosphate dehydrogenase (G6PD) levels. Peripheral smear shows the presence of bite cells and Heinz bodies. Which of the following is the most likely diagnosis in this patient?
Practice by Chapter
Liver pathology (hepatitis, cirrhosis)
Practice Questions
Gallbladder and biliary tract disorders
Practice Questions
Pancreatic diseases
Practice Questions
Kidney diseases
Practice Questions
Male reproductive pathology
Practice Questions
Female reproductive pathology
Practice Questions
Breast pathology
Practice Questions
Endocrine pathology
Practice Questions
Bone and joint pathology
Practice Questions
Skeletal muscle diseases
Practice Questions
Peripheral nerve disorders
Practice Questions
Soft tissue tumors
Practice Questions
Head and neck pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app