
Systemic Pathology — MCQs

On this page
A 56-year-old African American woman comes to the physician because of frequent urination. For the past year, she has had to urinate multiple times every hour. She has been thirstier and hungrier than usual. She has not had any pain with urination. She has no time to exercise because she works as an accountant. Her diet mostly consists of pizza and cheeseburgers. Her vital signs are within normal limits. Physical examination shows no abnormalities. Today, her blood glucose level is 200 mg/dL and her hemoglobin A1c is 7.4%. Urinalysis shows microalbuminuria. Which of the following is the most likely cause of this patient's proteinuria?
A 67-year-old man comes to the emergency department for the evaluation of two episodes of red urine since this morning. He has no pain with urination. He reports lower back pain and fever. Six months ago, he was diagnosed with osteoarthritis of the right knee that he manages with 1–2 tablets of ibuprofen per day. He has smoked one pack of cigarettes daily for the past 45 years. He does not drink alcohol. His temperature is 38.5°C (101.3°F), pulse is 95/min, and blood pressure is 130/80 mm Hg. Physical examination shows faint, diffuse maculopapular rash, and bilateral flank pain. The remainder of the examination shows no abnormalities. Urinalysis shows: Blood +3 Protein +1 RBC 10–12/hpf RBC cast negative Eosinophils numerous Which of the following is the most likely diagnosis?
A 12-year-old boy who recently immigrated from Namibia is being evaluated for exertional shortness of breath and joint pain for the past month. His mother reports that he used to play soccer but now is unable to finish a game before he runs out of air or begins to complain of knee pain. He was a good student but his grades have recently been declining over the past few months. The mother recalls that he had a sore throat and didn't go to school for 3 days a few months ago. He had chickenpox at the age of 5 and suffers from recurrent rhinitis. He is currently taking over-the-counter multivitamins. His blood pressure is 110/90 mm Hg, pulse rate is 55/min, and respiratory rate is 12/min. On physical examination, subcutaneous nodules are noted on his elbows bilaterally. On cardiac auscultation, a holosystolic murmur is heard over the mitral area that is localized. Lab work shows: Hemoglobin 12.9 g/dL Hematocrit 37.7% Leukocyte count 5,500/mm3 Neutrophils 65% Lymphocytes 30% Monocytes 5% Mean corpuscular volume 82.2 fL Platelet count 139,000/mm3 Erythrocyte sedimentation rate 35 mm/h C-reactive protein 14 mg/dL Antistreptolysin O (ASO) 400 IU (normal range: < 200 IU) Which is the mechanism behind the cause of this boy's symptoms?
A 46-year-old man diagnosed with pancreatic adenocarcinoma is admitted with fever, malaise, and dyspnea. He says that symptoms onset 2 days ago and have progressively worsened. Past medical history is significant for multiple abdominal surgeries including stenting of the pancreatic duct. Current inpatient medications are rosuvastatin 20 mg orally daily, aspirin 81 mg orally daily, esomeprazole 20 mg orally daily, oxycontin 10 mg orally twice daily, lorazepam 2 mg orally 3 times daily PRN, and ondansetron 10 mg IV. On admission, his vital signs include blood pressure 105/75 mm Hg, respirations 22/min, pulse 90/min, and temperature 37.0°C (98.6°F). On his second day after admission, the patient acutely becomes obtunded. Repeat vital signs show blood pressure 85/55 mm Hg, respirations 32/min, pulse 115/min. Physical examination reveals multiple ecchymoses on the trunk and extremities and active bleeding from all IV and venipuncture sites. There is also significant erythema and swelling of the posterior aspect of the left leg. Laboratory findings are significant for thrombocytopenia, prolonged PT and PTT, and an elevated D-dimer. Blood cultures are pending. Which of the following is most likely responsible for this patient’s current condition?
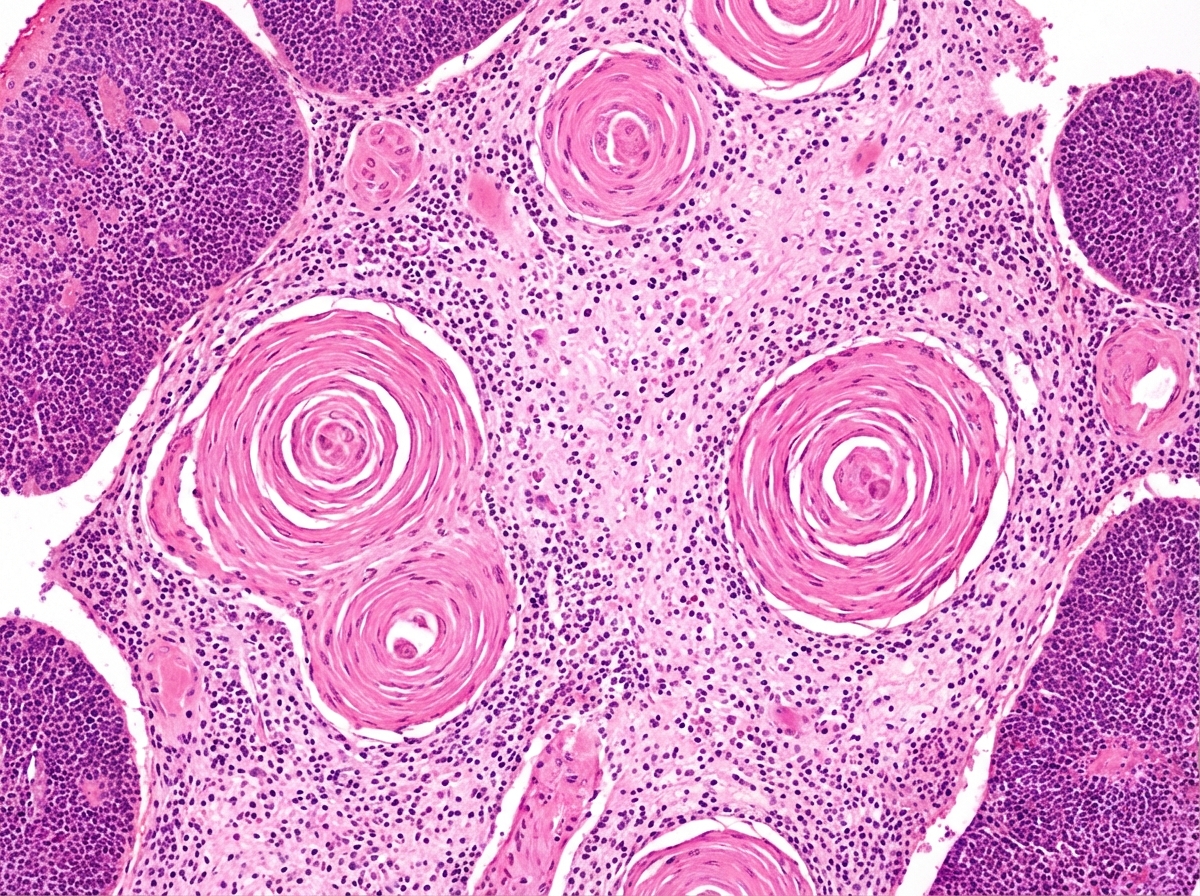
A section from the thymus of a patient with myasthenia gravis is examined (see image). The function of the portion of the thymus designated by the arrow plays what role in the pathophysiology of this disease?
A pathologist receives a patient sample for analysis. Cells in the sample are first labeled with fluorescent antibodies and then passed across a laser beam in a single file of particles. The light scatter and fluorescent intensity of the particles are plotted on a graph; this information is used to characterize the sample. This laboratory method would be most useful to establish the diagnosis of a patient with which of the following?
A 15-year-old boy is brought to the physician because his urine has been pink since that morning. During the past 2 days, he has had a sore throat and difficulty swallowing. He also reports having a low-grade fever. He has no pain with urination or changes in urinary frequency. He has had 2 similar episodes involving a sore throat and pink urine over the past 2 years. His older sister has systemic lupus erythematosus. His temperature is 38.3°C (101°F), pulse is 76/min, and blood pressure is 120/80 mm Hg. Oral examination shows an erythematous pharynx and enlarged tonsils. The remainder of the examination shows no abnormalities. Laboratory studies show: Leukocyte count 20,000/mm3 Serum Urea nitrogen 8 mg/dL Creatinine 1.4 mg/dL Urine Blood 3+ Protein 1+ RBC 15–17/hpf with dysmorphic features RBC casts numerous Ultrasound of both kidneys shows no abnormalities. A renal biopsy is most likely to show which of the following findings?
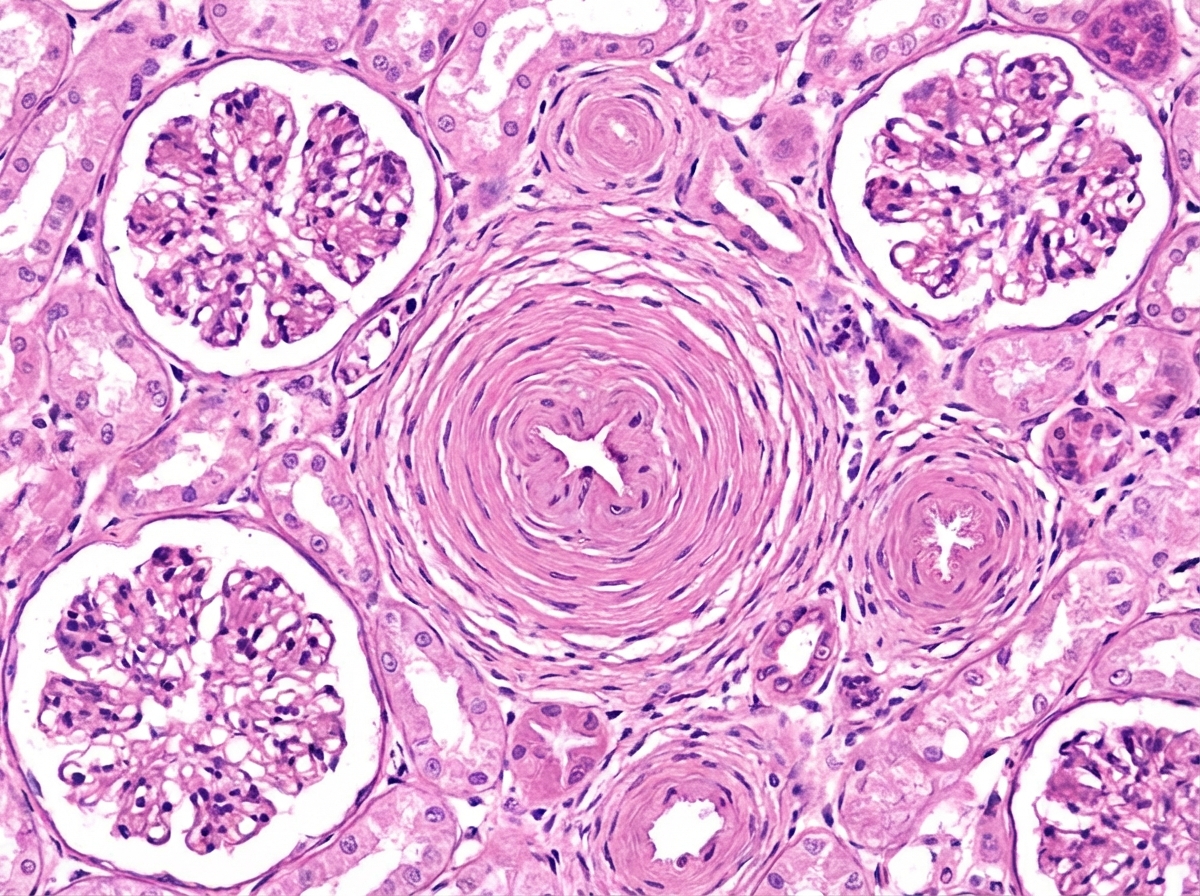
A 53-year-old man is brought to the emergency department by his wife because of a 1-day history of headache, blurry vision, and confusion. His wife also says that he hasn't urinated in the past 24 hours. Despite appropriate measures, the patient dies shortly after admission. A photomicrograph of a section of the kidney obtained at autopsy is shown. Which of the following is the most likely explanation for the findings indicated by the arrow?
A 17-year-old is brought to his primary care provider by his mother. They are concerned that his acne is getting worse and may leave scars. They have tried several over the counter products without success. He is otherwise healthy and without complaint. The boy was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines with some delay in reaching developmental milestones, especially in language development. He is having trouble with school and has a history of detentions for misbehavior and acting out. On examination, he stands 6 ft 3 inches tall, considerably taller than either parent or other family members with inflamed pustular acne on his face, shoulders, and chest. He is otherwise healthy. Which of the following karyotypes is most likely associated with this patient’s clinical features?
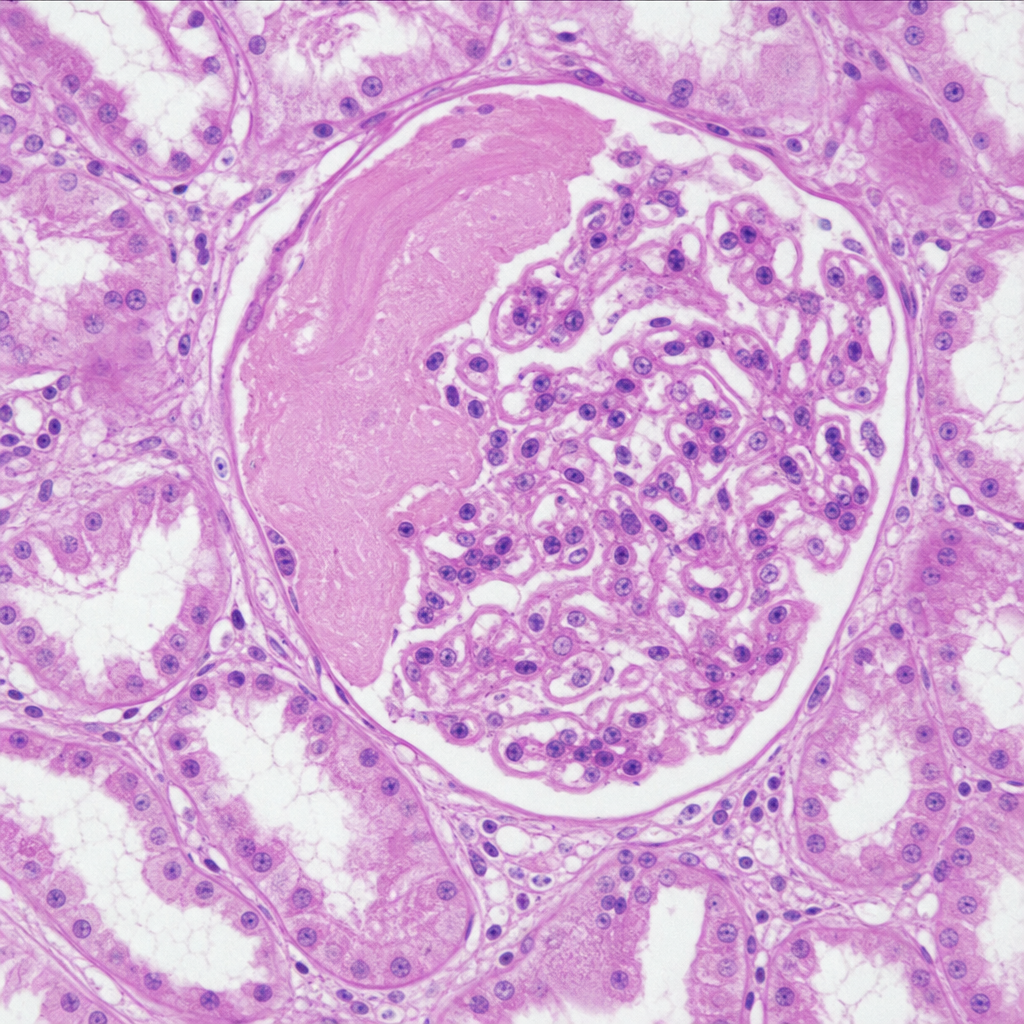
A 42-year-old man comes to the physician because of fatigue and decreased urination for the past 3 days. His creatinine is 2.5 mg/dL. A photomicrograph of a biopsy specimen of the right kidney is shown. Which of the following mechanisms most likely contributed to this patient's biopsy findings?
Practice by Chapter
Liver pathology (hepatitis, cirrhosis)
Practice Questions
Gallbladder and biliary tract disorders
Practice Questions
Pancreatic diseases
Practice Questions
Kidney diseases
Practice Questions
Male reproductive pathology
Practice Questions
Female reproductive pathology
Practice Questions
Breast pathology
Practice Questions
Endocrine pathology
Practice Questions
Bone and joint pathology
Practice Questions
Skeletal muscle diseases
Practice Questions
Peripheral nerve disorders
Practice Questions
Soft tissue tumors
Practice Questions
Head and neck pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app