
Systemic Pathology — MCQs

On this page
A 32-year-old woman is brought to your office by her husband. The husband says that she had been acting strange lately. She has been forgetful, and she sometimes becomes angered for no reason, which is highly unusual for her. She has also been having random, uncontrollable movements, which are also new. On examination, she appears withdrawn and flat. On further questioning, she reveals that her father died at age 45 from a movement disorder. Which of the following is the pathological hallmark of the patient's condition?
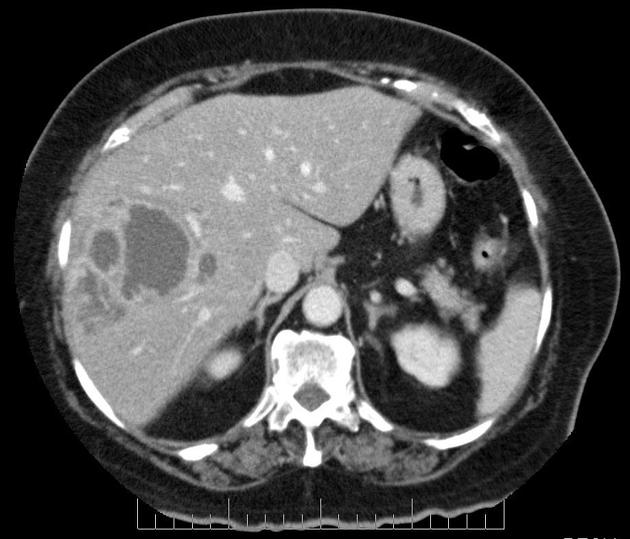
A 40-year-old man presents to the office with complaints of epigastric discomfort for the past 6 months. He adds that the discomfort is not that bothersome as it does not interfere with his daily activities. He does not have any other complaints at the moment. The past medical history is insignificant. He is a non-smoker and does not consume alcohol. He recently came back from a trip to South America where he visited a relative who owned a sheep farm. On physical examination, he has a poorly palpable epigastric non-tender mass with no organomegaly. The hepatitis B and C serology are negative. The liver CT scan and MRI are shown. What is the most likely diagnosis?
A 60-year-old African American woman presents to her family physician with shortness of breath on exertion. She also describes shortness of breath when she lies down to go to bed at night, as well as recent swelling in her ankles. Past medical history is significant for long-standing hypertension, for which she takes amlodipine and lisinopril. Her temperature is 36.8°C (98.2°F), the heart rate is 90/min, the respiratory rate is 15/min, and the blood pressure is 135/80 mm Hg. The physical exam is significant for JVD, lower extremity pitting edema, laterally displaced PMI, left ventricular heave, bilateral pulmonary crackles, and an S4 heart sound. Chest X-ray demonstrates pulmonary vascular congestion, Kerley B lines, and cardiomegaly. Echocardiogram demonstrates a preserved ejection fraction. Kidney biopsy would likely demonstrate which of the following?
A 65-year-old African-American woman comes to the physician because of severe lower back pain. She has had dull lower back pain for several months, which suddenly become sharp in nature after lifting a heavy bucket of water 2 days ago. The pain is midline and does not radiate. She has had frequent vaginal dryness and hot flashes since menopause at the age of 55 years, for which she is on hormone replacement therapy. She has hypertension, hypercholesterolemia, and hypothyroidism. Her other medications include hydrochlorothiazide, simvastatin, and levothyroxine. She attends a 30-minute power walking class twice a week. She has smoked a pack of cigarettes daily for 40 years. She does not drink alcohol. She does not appear in distress. She is 165 cm (5 ft 5 in) tall and weighs 75 kg (165 lb); her BMI is 27.6 kg/m2. Vital signs are within normal limits. Examination shows midline lumbar tenderness. Muscle strength is full and deep tendon reflexes are 2+. Straight-leg raising is negative but painful. MRI of the spine shows an acute compression fracture of the L3 vertebral body and an old compression fracture of the L4 vertebra. Which of the following parts of this patient's history is the strongest predisposing factor for her condition?
A 51-year-old woman with hyperlipidemia comes to the physician because of weakness for one month. At the end of the day, she feels too fatigued to cook dinner or carry a laundry basket up the stairs. She also complains of double vision after she reads for long periods of time. All of her symptoms improve with rest. Her only medication is pravastatin. Physical examination shows drooping of the upper eyelids. Strength is initially 5/5 in the upper and lower extremities but decreases to 4/5 after a few minutes of sustained resistance. Sensation to light touch is intact and deep tendon reflexes are normal. Which of the following best describes the pathogenesis of this patient's condition?
A 46-year-old man comes to the physician because of a 4-month history of progressively worsening fatigue and loss of appetite. Five years ago, he received a kidney transplant from a living family member. Current medications include sirolimus and mycophenolate. His blood pressure is 150/95 mm Hg. Laboratory studies show normocytic, normochromic anemia and a serum creatinine concentration of 3.1 mg/dL; his vital signs and laboratory studies were normal 6 months ago. Which of the following is the most likely underlying mechanism of this patient’s increase in creatinine concentration?
A 53-year-old woman presents to her physician for evaluation of sudden onset respiratory distress for the past few hours. The past medical history includes a myocardial infarction 2 years ago. The vital signs include a blood pressure 70/40 mm Hg, pulse 92/min, respiratory rate 28/min, and SpO2 92% on room air. The physical examination reveals bilateral basal crepitations on auscultation. The echocardiogram reveals an ejection fraction of 34%. She is admitted to the medical floor and started on furosemide. The urine output in 24 hours is 400 mL. The blood urea nitrogen is 45 mg/dL and the serum creatinine is 1.85 mg/dL. The fractional excretion of sodium is 2.4%. Urinalysis revealed muddy brown granular casts. Which of the following is the most likely cause of the abnormal urinalysis?
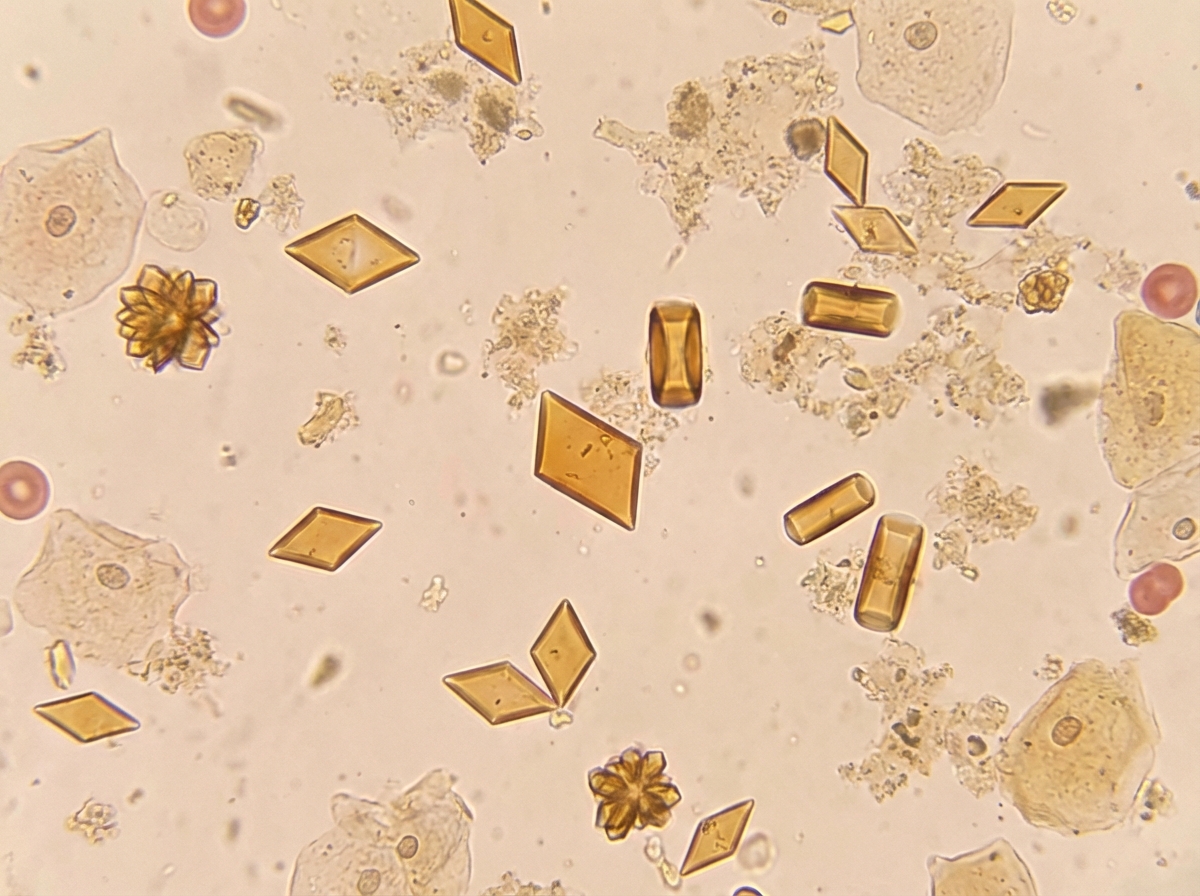
A 45-year-old woman presents with severe, acute-onset colicky abdominal pain and nausea. She also describes bone pain, constipation, headache, decreased vision, and menstrual irregularity. Past medical history is significant for surgical removal of an insulinoma one year ago. Two months ago, she was prescribed fluoxetine for depression but hasn't found it very helpful. Family history is significant for a rare genetic syndrome. Non-contrast CT, CBC, CMP, and urinalysis are ordered in the diagnostic work-up. Urine sediment is significant for the findings shown in the picture. Which of the following will also be a likely significant finding in the diagnostic workup?
An autopsy of a patient's heart who recently died in a motor vehicle accident shows multiple nodules near the line of closure on the ventricular side of the mitral valve leaflet. Microscopic examination shows that these nodules are composed of immune complexes, mononuclear cells, and thrombi interwoven with fibrin strands. These nodules are most likely to be found in which of the following patients?
A 32-year-old man presents with a history of diarrhea several days after eating a hot dog at a neighborhood barbeque. He notes that the diarrhea is visibly bloody, but he has not experienced a fever. He adds that several other people from his neighborhood had similar complaints, many of which required hospitalization after eating food at the same barbeque. His temperature is 37°C (98.6°F ), respiratory rate is 16/min, pulse is 77/min, and blood pressure is 100/88 mm Hg. A physical examination is performed and is within normal limits. Blood is drawn for laboratory testing. The results are as follows: Hb%: 12 gm/dL Total count (WBC): 13,100/mm3 Differential count: Neutrophils: 80% Lymphocytes: 15% Monocytes: 5% ESR: 10 mm/hr Glucose, Serum: 90 mg/dL BUN: 21 mg/dL Creatinine, Serum: 1.96 mg/dL Sodium, Serum: 138 mmol/L Potassium, Serum: 5.2 mmol/L Chloride, Serum: 103 mmol/L Bilirubin, Total: 2.5 mg/dL Alkaline Phosphatase, Serum: 66 IU/L Aspartate aminotransferase (AST): 32 IU/L Alanine aminotransferase (ALT): 34 IU/L Urinalysis is normal except for RBC casts. What is the most concerning possible complication?
Practice by Chapter
Liver pathology (hepatitis, cirrhosis)
Practice Questions
Gallbladder and biliary tract disorders
Practice Questions
Pancreatic diseases
Practice Questions
Kidney diseases
Practice Questions
Male reproductive pathology
Practice Questions
Female reproductive pathology
Practice Questions
Breast pathology
Practice Questions
Endocrine pathology
Practice Questions
Bone and joint pathology
Practice Questions
Skeletal muscle diseases
Practice Questions
Peripheral nerve disorders
Practice Questions
Soft tissue tumors
Practice Questions
Head and neck pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app