
Systemic Pathology — MCQs

On this page
An 18-year-old African-American woman comes to the physician for the evaluation of worsening fatigue that started 1 year ago. Physical examination shows mild jaundice and splenomegaly. Laboratory studies show: Hemoglobin 10.4 g/dL Mean corpuscular hemoglobin concentration 43% Hb/cell Platelet count 220,000/mm3 Reticulocyte count 7% A peripheral blood smear shows target cells and erythrocytes with hemoglobin crystals. Which of the following is the most likely underlying cause of this patient's findings?
A 34-year-old female presents to her primary care physician with complaints of fevers, nausea/vomiting, and severe left flank pain that has developed over the past several hours. She denies any prior episodes similar to her current presentation. Physical examination is significant for a body temperature of 39.1 C and costovertebral angle tenderness. A urinalysis and urine microscopy are ordered. Which of the following findings on kidney histology would be expected in this patient?
A 12-year-old girl is presented to the office by her mother with complaints of cola-colored urine and mild facial puffiness that began 5 days ago. According to her mother, she had a sore throat 3 weeks ago. Her immunization records are up to date. The mother denies fever and any change in bowel habits. The vital signs include blood pressure 138/78 mm Hg, pulse 88/min, temperature 36.8°C (98.2°F), and respiratory rate 11/min. On physical examination, there is pitting edema of the upper and lower extremities bilaterally. An oropharyngeal examination is normal. Urinalysis shows the following results: pH 6.2 Color dark brown Red blood cell (RBC) count 18–20/HPF White blood cell (WBC) count 3–4/HPF Protein 1+ Cast RBC casts Glucose absent Crystal none Ketone absent Nitrite absent 24 h urine protein excretion 0.6 g HPF: high-power field Which of the following would best describe the light microscopy findings in this case?
A 7-year-old girl is brought to the physician with complaints of erythema and rashes over the bridge of her nose and on her forehead for the past 6 months. She also has vesiculobullous and erythematous scaly crusted lesions on the scalp and around the perioral areas. Her parents report a history of worsening symptoms during exposure to sunlight, along with a history of joint pain and oral ulcers. Her temperature is 38.6°C (101.4°F), pulse is 88/min, and respirations are 20/min. On physical examination, pallor and cervical lymphadenopathy are present. On cutaneous examination, diffuse hair loss and hyperpigmented scaly lesions are present. Her laboratory studies show: Hemoglobin 7.9 mg/dL Total leukocyte count 6,300/mm3 Platelet count 167,000/mm3 Erythrocyte sedimentation rate 30 mm/h ANA titer 1:520 (positive) Which of the following most likely explains the mechanism of this condition?
Physical exam of a 15-year-old female reveals impetigo around her mouth. A sample of the pus is taken and cultured. Growth reveals gram-positive cocci in chains that are bacitracin sensitive. Which of the following symptoms would be concerning for a serious sequela of this skin infection?
A 19-year-old male from rural West Virginia presents to his family medicine doctor to discuss why he is having trouble getting his wife pregnant. On exam, he is 6 feet 2 inches with a frail frame and broad hips for a male his size. He is noted to have mild gynecomastia, no facial hair, and small, underdeveloped testes. He claims that although he has a lower libido than most of his friends, he does have unprotected sex with his wife. His past medical history is notable for developmental delay and difficulties in school. What is the most likely chromosomal abnormality in this patient?
A 42-year-old woman comes to the physician because of a 2-month history of progressive muscular weakness. She has had difficulty climbing stairs, getting up from chairs, and brushing her hair. Her vital signs are within normal limits. Muscle strength is 2/5 with flexion of the hips and 3/5 with abduction of the shoulders. She is unable to stand up from her chair without the use of her arms for support. Laboratory studies show elevations in leukocyte count, erythrocyte sedimentation rate, and creatine kinase concentration. Histological evaluation of a biopsy specimen of the deltoid muscle is most likely to show which of the following?
A 20-year-old man presents with a painless neck mass that has gradually increased in size. The mass is anteromedial to the right sternocleidomastoid muscle and has been present for 3 years. The mass increased in size and became more tender following an upper respiratory infection. An ultrasound of the neck identifies a single, round cystic mass with uniform, low echogenicity, and no internal septations. A contrast-enhanced CT scan of the neck shows a homogeneous mass with low attenuation centrally and with smooth rim enhancement. Which of the following is the most likely diagnosis?
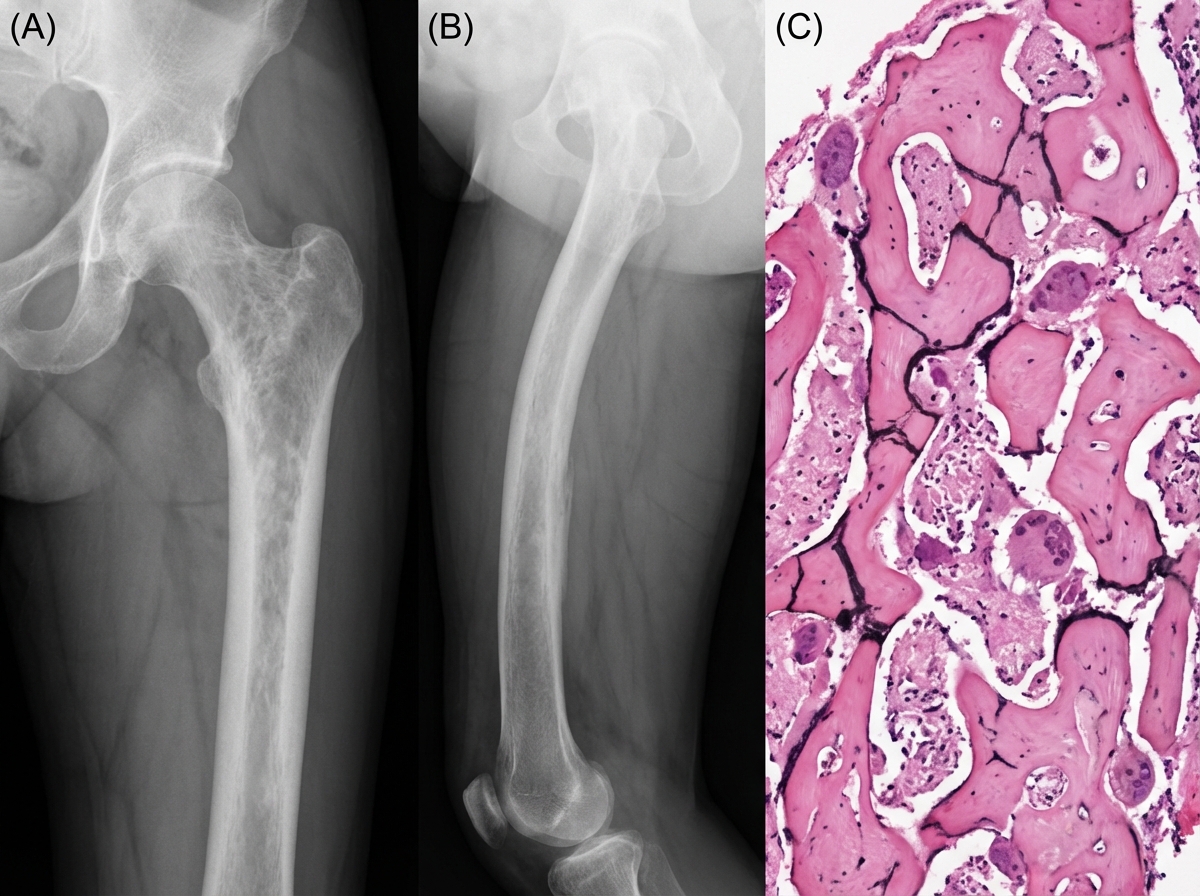
A 55-year-old male presents with left hip pain and stiffness. Radiographs are shown in Figures A and B. Serum alkaline phosphatase levels are elevated. A biopsy of the left femur is performed and shown in Figure C. Which of the following cells are initially responsible for this condition?
Following a recent myocardial infarction, a 60-year-old woman has been started on multiple medications at the time of discharge from the hospital. After 10 days of discharge, she presents to the emergency department with a history of fever, headache, and dark colored urine for 2 days. Her husband mentions that she has not passed urine for the last 24 hours. Her physical examination shows significant pallor, and multiple petechiae are present all over her limbs. Her vital signs include: temperature 38.9°C (102.0°F), pulse rate 94/min, blood pressure 124/82 mm Hg, and respiratory rate 16/min. Her sensorium is altered with the absence of spontaneous speech and spontaneous movements. She responds inappropriately to verbal stimuli. Her laboratory results show the presence of anemia and thrombocytopenia. Examination of peripheral blood smear shows the presence of schistocytes. Serum creatinine is 2 mg/dL. Serum levels of fibrinogen, fibrin monomers, fibrin degradation products and D-dimers are normal. Prothrombin time (PT) and activated partial thromboplastin time (aPTT) are normal. Which is the most likely treatment for this patient’s condition?
Practice by Chapter
Liver pathology (hepatitis, cirrhosis)
Practice Questions
Gallbladder and biliary tract disorders
Practice Questions
Pancreatic diseases
Practice Questions
Kidney diseases
Practice Questions
Male reproductive pathology
Practice Questions
Female reproductive pathology
Practice Questions
Breast pathology
Practice Questions
Endocrine pathology
Practice Questions
Bone and joint pathology
Practice Questions
Skeletal muscle diseases
Practice Questions
Peripheral nerve disorders
Practice Questions
Soft tissue tumors
Practice Questions
Head and neck pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app