
Human T-cell leukemia virus — MCQs

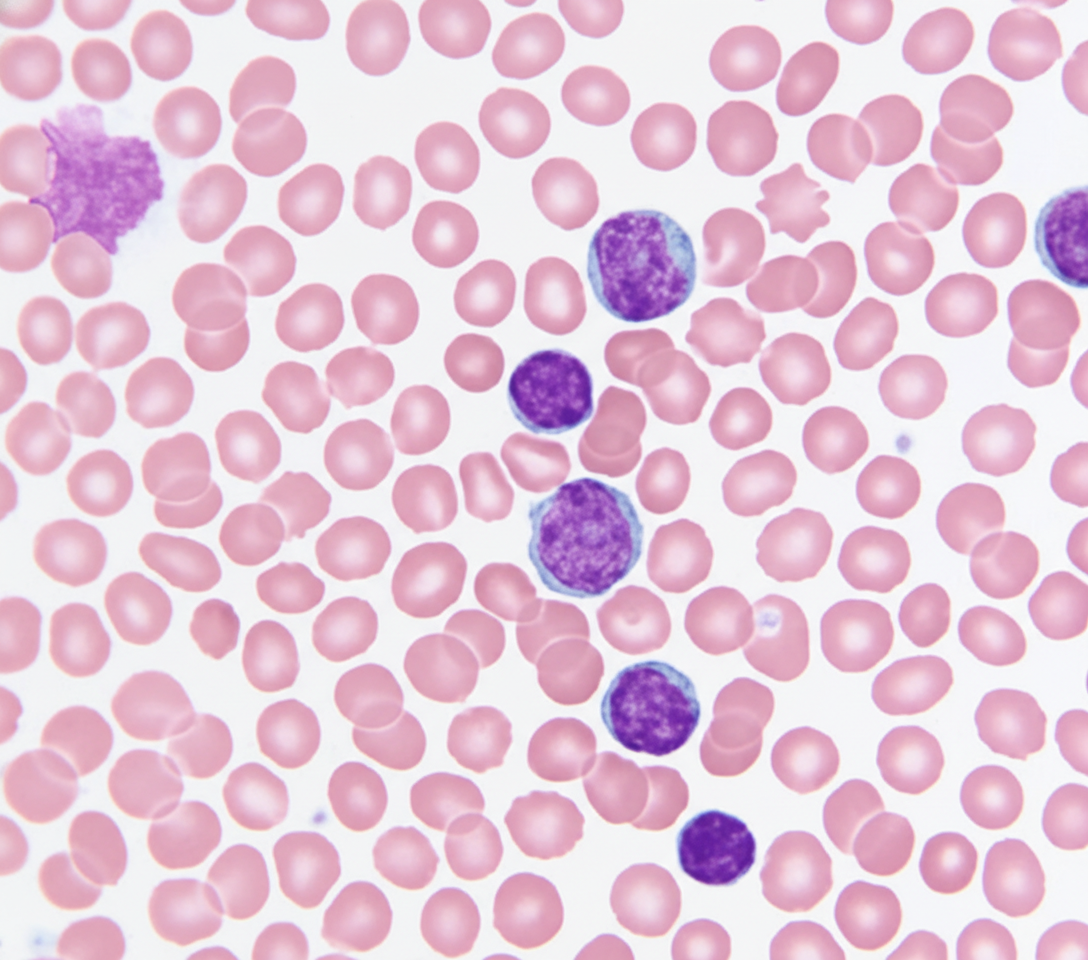
A 69-year-old Caucasian man presents for a routine health maintenance examination. He feels well. He has no significant past medical history. He takes aspirin for the occasional headaches that he has had for over several years. He exercises every day and does not smoke. His father was diagnosed with a hematologic malignancy at 79 years old. The patient’s vital signs are within normal limits. Physical examination shows no abnormalities. The laboratory test results are as follows: Hemoglobin 14.5 g/dL Leukocyte count 62,000/mm3 Platelet count 350,000/mm3 A peripheral blood smear is obtained (shown on the image). Which of the following best explains these findings?
A 5-year-old boy presents to his pediatrician with weakness. His father observed that his son seemed less energetic at daycare and kindergarten classes. He was becoming easily fatigued from mild play. His temperature is 98°F (37°C), blood pressure is 90/60 mmHg, pulse is 100/min, and respirations are 20/min. Physical exam reveals pale conjunctiva, poor skin turgor and capillary refill, and cervical and axillary lymphadenopathy with assorted bruises throughout his body. A complete blood count reveals the following: Leukocyte count: 3,000/mm^3 Segmented neutrophils: 30% Bands: 5% Eosinophils: 5% Basophils: 10% Lymphocytes: 40% Monocytes: 10% Hemoglobin: 7.1 g/dL Hematocrit: 22% Platelet count: 50,000/mm^3 The most specific diagnostic assessment would most likely show which of the following?
A 4-year-old girl is brought to the physician because of a 3-week history of generalized fatigue and easy bruising. During the past week, she has also had fever and severe leg pain that wakes her up at night. Her temperature is 38.3°C (100.9°F), pulse is 120/min, and respirations are 30/min. Examination shows cervical and axillary lymphadenopathy. The abdomen is soft and nontender; the liver is palpated 3 cm below the right costal margin, and the spleen is palpated 2 cm below the left costal margin. Laboratory studies show: Hemoglobin 10.1 g/dL Leukocyte count 63,000/mm3 Platelet count 27,000/mm3 A bone marrow aspirate predominantly shows immature cells that stain positive for CD10, CD19, and TdT. Which of the following is the most likely diagnosis?
A 72-year-old man goes to his primary care provider for a checkup after some blood work showed lymphocytosis 3 months ago. He says he has been feeling a bit more tired lately but doesn’t complain of any other symptoms. Past medical history is significant for hypertension and hyperlipidemia. He takes lisinopril, hydrochlorothiazide, and atorvastatin. Additionally, his right hip was replaced three years ago due to osteoarthritis. Family history is noncontributory. He drinks socially and does not smoke. Today, he has a heart rate of 95/min, respiratory rate of 17/min, blood pressure of 135/85 mm Hg, and temperature of 36.8°C (98.2°F). On physical exam, he looks well. His heartbeat has a regular rate and rhythm and lungs that are clear to auscultation bilaterally. Additionally, he has mild lymphadenopathy of his cervical lymph nodes. A complete blood count with differential shows the following: Leukocyte count 5,000/mm3 Red blood cell count 3.1 million/mm3 Hemoglobin 11.0 g/dL MCV 95 um3 MCH 29 pg/cell Platelet count 150,000/mm3 Neutrophils 40% Lymphocytes 40% Monocytes 5% A specimen is sent for flow cytometry that shows a population that is CD 5, 19, 20, 23 positive. Which of the following is the most likely diagnosis?
A 72-year-old man presents to the primary care clinic for evaluation of progressive fatigue and weight loss. His past medical history is significant for hypercholesterolemia, type 2 diabetes mellitus, aortic stenosis, and chronic renal insufficiency. He endorses being well-rested after waking from sleep but fatiguing rapidly during the day. In addition, he states that he has lost 15lbs over the previous month. His temperature is 98.3°F (36.8°C), pulse is 100/min, blood pressure is 110/85 mmHg, respirations are 16/min, and oxygen saturation is 96% on room air. Physical exam is notable for conjunctival pallor and scattered areas of ecchymoses. His laboratory results are shown below: Serum: Na+: 140 mEq/L K+: 4.0 mEq/L Cl-: 101 mEq/L HCO3-: 22 mEq/L BUN: 30 mg/dL Glucose: 160 mg/dL Creatinine: 1.9 mg/dL Leukocyte count: 1,100/mm^3 Absolute neutrophil count 920/mm^3 Hemoglobin 8.4 g/dL Platelet count: 45,000/mm^3 Mean corpuscular hemoglobin concentration: 34% Red blood cell distribution width: 12.0% Mean corpuscular volume: 92 µm^3 Lactate dehydrogenase: 456 IU/L Haptoglobin 120 mg/dL Fibrinogen 214 mg/dL A bone marrow biopsy is performed which shows cells that are CD19+, CD20+, CD11c+, and stain with acid phosphatase 5 and tartrate-resistant. Which of the following is the next best step in the treatment of his disorder?
A 29-year-old man comes to the physician because of a 3-month history of fatigue, weight loss, and multiple painless swellings on his neck and axilla. He reports that his swellings become painful after he drinks alcohol. Physical examination shows nontender cervical and axillary lymphadenopathy. A lymph node biopsy specimen shows giant binucleate cells. Which of the following is the most likely diagnosis?
A 16-year-old boy is brought to the physician because of a lesion that has been growing on his jaw over the past several months. He recently immigrated to the USA from Kenya with his family. Physical examination shows a 3-cm solid mass located above the left mandible. There is cervical lymphadenopathy. Biopsy of the mass shows sheets of lymphocytes and interspersed reactive histiocytes with abundant, clear cytoplasm and phagocytosed debris. Which of the following mechanisms is most likely directly responsible for the malignant transformation of this patient's cells?
A 40-year-old male presents to his primary care physician for a regularly scheduled check-up. Physical examination reveals nontender cervical lymphadenopathy. A biopsy of the lymph node reveals aggregates of follicular architecture, and cytogenic analysis shows a t(14;18) translocation. The protein most likely responsible for the patient’s condition does which of the following:
A 55-year-old man comes to the physician because of a 3-day history of decreased urine output, progressively worsening bilateral pedal edema, and fatigue. He has a 4-month history of persistent lower back pain. He has hypercholesterolemia and stable angina pectoris. Current medications include atorvastatin, aspirin, and ibuprofen. His pulse is 80/min, respirations are 16/min, and blood pressure is 150/100 mm Hg. Examination shows periorbital and pedal edema and pallor. There is tenderness of the lumbar spinal vertebrae. Straight leg raise test is negative. The remainder of the examination shows no abnormalities. Laboratory studies show: Hemoglobin 8.9 g/dl Serum Urea nitrogen 20 mg/dl Creatinine 2.4 mg/dl Calcium 11.2 mg/dl Alkaline phosphatase 140 U/L X-ray of the spine shows diffuse osteopenia and multiple lytic lesions. Which of the following is most likely to confirm the diagnosis?
A 63-year-old man presents to his primary care physician because he has been having headaches and hearing loss. In addition, he says that he has been having difficulty opening his jaw to eat and recurrent middle ear infections. Physical exam reveals enlarged neck lymph nodes and a mass in the nasopharynx. Biopsy of the mass reveals undifferentiated squamous epithelial cells. The organism that is most likely associated with this patient's disease is also associated with which of the following disorders?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app