
Gram-negative — MCQs

On this page
An investigator is studying the growth of an organism in different media. The organism is inoculated on a petri dish that contains heated sheep blood, vancomycin, nystatin, trimethoprim, and colistin. The resulting growth medium is incubated at 37°C. Numerous small, white colonies are seen after incubation for 48 hours. This organism is most likely to cause which of the following conditions?
A 13-year-old boy is brought by his mother to the emergency department because he has had fever, chills, and severe coughing for the last two days. While they originally tried to manage his condition at home, he has become increasingly fatigued and hard to arouse. He has a history of recurrent lung infections and occasionally has multiple foul smelling stools. On presentation, his temperature is 102.2 °F (39 °C), blood pressure is 106/71 mmHg, pulse is 112/min, and respirations are 20/min. Physical exam reveals scattered rhonchi over both lung fields, rales at the base of the right lung base and corresponding dullness to percussion. The most likely organism responsible for this patient's symptoms has which of the following characteristics?
A 21-year-old man presents to the emergency department with a 1-week history of increasing knee pain. Specifically, he says that the pain is severe enough that he is no longer able to bend his knee. His past medical history is not significant, but he says that he is sexually active with multiple partners. On physical exam, his right knee is found to be swollen, erythematous, and tender to palpation. Laboratory testing demonstrates an elevated erythrocyte sedimentation rate and C-reactive protein. Which of the following properties describes the organism that is most likely responsible for this patient's symptoms?
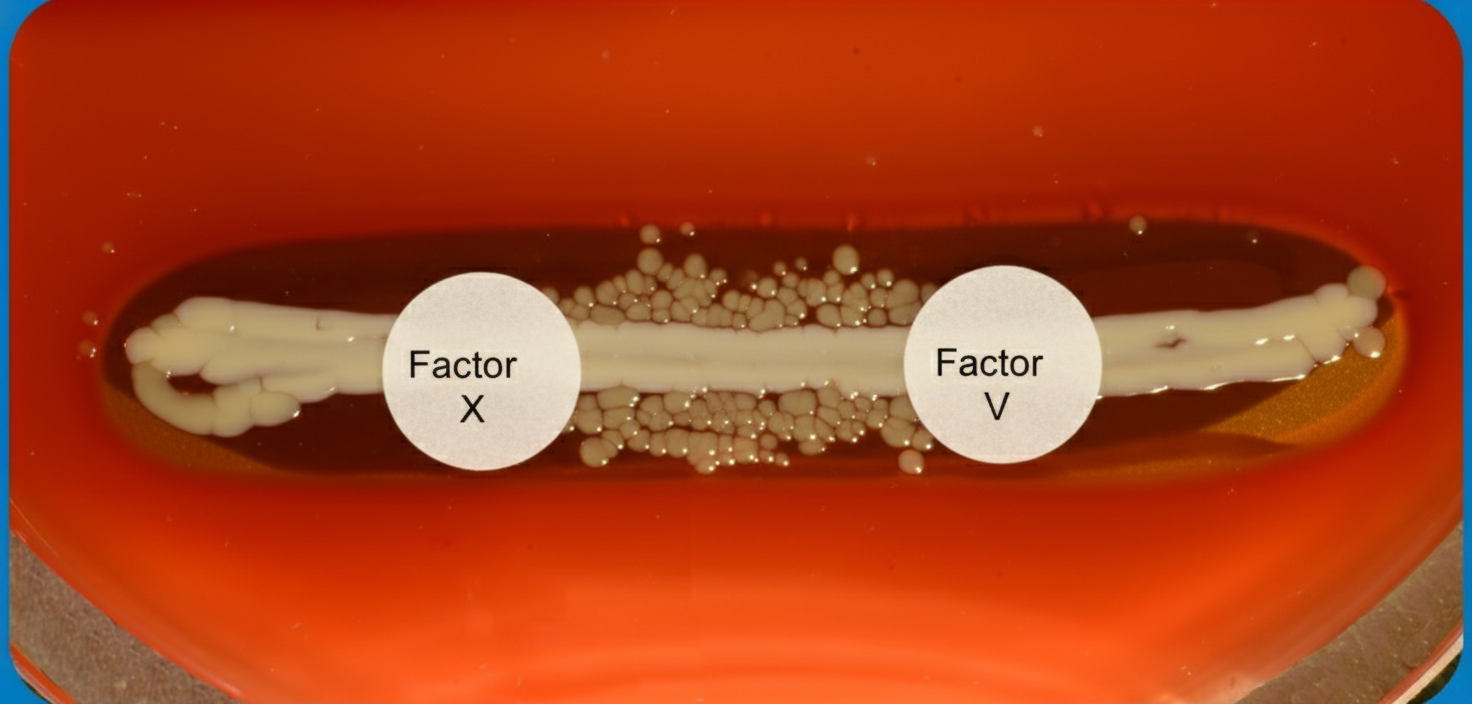
A 6-month old child is brought to the ER by parents for one day of fever, decreased feeding, and lethargy. They report that neither she nor her siblings are immunized due to their concerns about vaccinations. On exam, the infant is toxic-appearing. Antibiotics are started and lumbar puncture reveals bacterial meningitis caused by a gram-negative, encapsulated organism that requires chocolate agar and the two factors shown in Image A for growth. Which organism does this best describe?
A 39-year-old man presents to his primary care physician with a 10-hour history of severe diarrhea. He says that he was recently at a company picnic and after returning home he began to experience severe watery diarrhea. He says that the diarrhea was accompanied by nausea and abdominal pain. His physician informs him that he was likely infected by a lactose-fermenting, gram-negative organism. Which of the following changes would be seen in a cell that was affected by the heat stable toxin produced by this organism?
A 42-year-old homeless male presents with fever and cough. He was found unconscious on the side of the road and was brought to the emergency room. He is noticeably drunk and is unable to answer any questions. On physical exam his temperature is 103°F (40°C), blood pressure is 130/85 mmHg, pulse is 110/min, respirations are 23/min, and pulse oximetry is 96% on room air. You note decreased breath sounds in the right lower lobe. The pathogen most likely responsible for this patient's symptoms has which of the following features?
A 53-year-old man presents to your Louisiana gulf coast community hospital with 48 hours of profuse watery diarrhea and 24 hours of vomiting and chills. The patient has a past medical history significant for hypertension and hypercholesterolemia. The patient denies sick contacts or any interaction with animals for the last month. Two days ago the patient attended a family crawfish boil where oysters, boiled crabs, and crawfish were consumed. Stool occult blood was negative. What is the most likely etiology of the patient's symptoms?
A 24-year-old man presents to the office, complaining of a rash and “not feeling well.” The patient reports fatigue, a headache, and a possible fever. He says he has felt this way since a camping trip with his family in North Carolina, but he denies any contact with sick individuals. On examination, his vital signs include: temperature 38.5°C (101.3°F), blood pressure 100/60 mm Hg, heart rate 82 beats per minute, respiratory rate 14 breaths per minute, and O2 saturation 99% on room air. The patient appears unwell. He has a maculopapular rash on his upper and lower extremities, including the palms of his hands and soles of his feet. He says he started feeling sick a few days before he got the rash, which prompted him to come into the office. The patient denies itching but admits to some nausea and vomiting. He also admits to unprotected sex with a single female partner for the past three years. What is the most likely causative agent of this patient’s presentation?
A 2-year-old boy is brought to the physician because of fever, productive cough, and shortness of breath. Since birth, he has had multiple respiratory infections requiring treatment with antibiotics. His immunizations are up-to-date. He is in the 10th percentile for height and weight. His temperature is 38°C (100.3°F). Examination detects diffuse bilateral wheezing and cervical lymphadenopathy. Flow cytometric analysis of a serum sample from the patient fails to fluoresce after incubation with dihydrorhodamine. This patient is at greatest risk of infection with which of the following organisms?
A 29-year-old woman presents to her primary care provider complaining of lower back pain. She reports a 3 day history of extreme right lower back pain. She also reports mild dysuria. Her past medical history is notable for recurrent urinary tract infections leading to 3 emergency room visits over the past year. Her family history is notable for renal cell carcinoma in her paternal grandfather and diabetes in her father. Her temperature is 99.5°F (37.5°C), blood pressure is 125/75 mmHg, pulse is 82/min, and respirations are 18/min. On exam, she has mild right costovertebral angle tenderness. Radiography demonstrates a vague radiopaque structure in the right lower abdomen. Results of a urinalysis are shown below: Appearance: Hazy, yellow Protein: Negative Specific gravity: 1.029 WBC: 2+ Casts: None Bacteria: None pH: 8.9 Blood: Negative Bilirubin: Negative Urobilinogen: < 2.0 A urine culture is pending. Which of the following pathogens is most likely responsible for this patient’s condition?
Practice by Chapter
Neisseria species (meningitidis, gonorrhoeae)
Practice Questions
Escherichia coli
Practice Questions
Klebsiella species
Practice Questions
Proteus species
Practice Questions
Pseudomonas aeruginosa
Practice Questions
Haemophilus influenzae
Practice Questions
Bordetella pertussis
Practice Questions
Legionella pneumophila
Practice Questions
Bacteroides and anaerobic gram-negatives
Practice Questions
Helicobacter pylori
Practice Questions
Campylobacter jejuni
Practice Questions
Vibrio species
Practice Questions
ESBL and CRE pathogens
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app