
Gram-negative — MCQs

On this page
A 39-year-old man presents with a 4-week history of painless, non-discharging lesions on his penis and scrotum. He was diagnosed with chronic myeloid leukemia two years ago and treated with imatinib. He currently takes no medications. He has a 20-pack-year smoking history and drinks 1-2 beers on weekends. He reports unprotected intercourse with a woman while traveling abroad 4 months ago. His temperature is 37°C, pulse is 85/min, and blood pressure is 128/82 mm Hg. Examination reveals three non-tender lesions, each approximately 1 cm in size, on his genitalia. There is no inguinal lymphadenopathy. Which of the following is the most likely causative organism?
Four days after being admitted to the hospital for widespread second-degree burns over his arms and thorax, a 29-year-old man develops a fever and wound discharge. His temperature is 38.8°C (101.8°F). Examination shows a discolored burn eschar with edema and redness of the surrounding skin. The wounds have a sickly, sweet odor. A culture of the affected tissue grows an aerobic, gram-negative rod. The causal pathogen most likely produces which of the following substances?
A previously healthy 29-year-old man comes to the emergency department for a 2-day history of abdominal pain, vomiting, and watery diarrhea. Bowel movements occur every 3 hours and are non-bloody. He recently returned from a backpacking trip in Central America. He does not take any medications. Stool culture shows gram-negative, rod-shaped bacteria that ferment lactose. Which of the following toxins is most likely to be involved in the pathogenesis of this patient's symptoms?
A 3-day-old boy is brought to the physician by his mother because of irritability and feeding intolerance for 1 day. His temperature is 39.2°C (102.6°F). Physical examination shows a bulging anterior fontanelle. A photomicrograph of a Gram stain of the cerebrospinal fluid is shown. Further evaluation shows that the organism expresses the K1 capsular polysaccharide. Which of the following is the most likely causal pathogen?
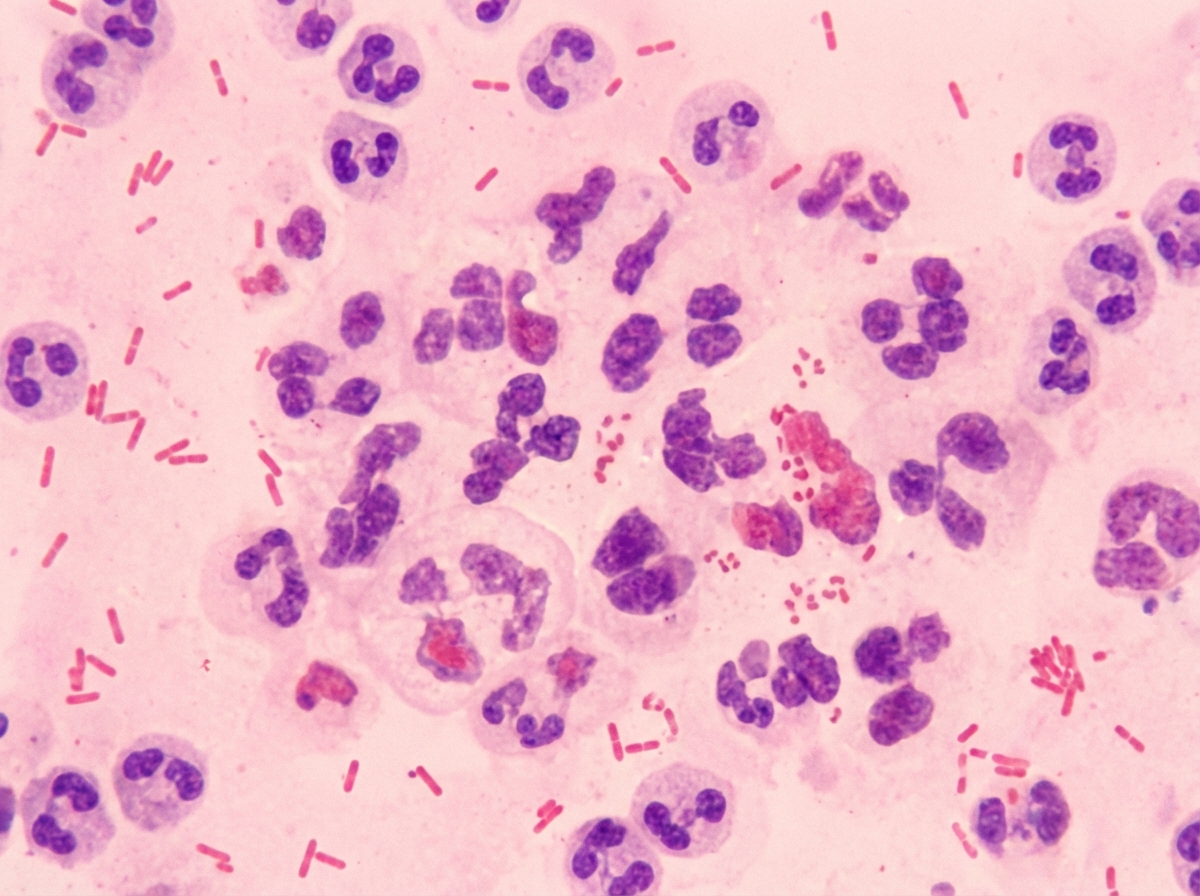
A 24-year-old woman presents to the ED with symptoms of pelvic inflammatory disease despite being previously treated with azithromycin for chlamydial infection. Based on your clinical understanding about the epidemiology of PID, you decide to obtain a gram stain which shows a gram-negative diplococci. What is the next step in order to confirm the identity of the organism described?
A 25-day-old male infant presents to the emergency department because his mother states that he has been acting irritable for the past 2 days and has now developed a fever. On exam, the infant appears uncomfortable and has a temperature of 39.1 C. IV access is immediately obtained and a complete blood count and blood cultures are drawn. Lumbar puncture demonstrates an elevated opening pressure, elevated polymorphonuclear neutrophil, elevated protein, and decreased glucose. Ampicillin and cefotaxime are immediately initiated and CSF culture eventually demonstrates infection with a Gram-negative rod. Which of the following properties of this organism was necessary for the infection of this infant?
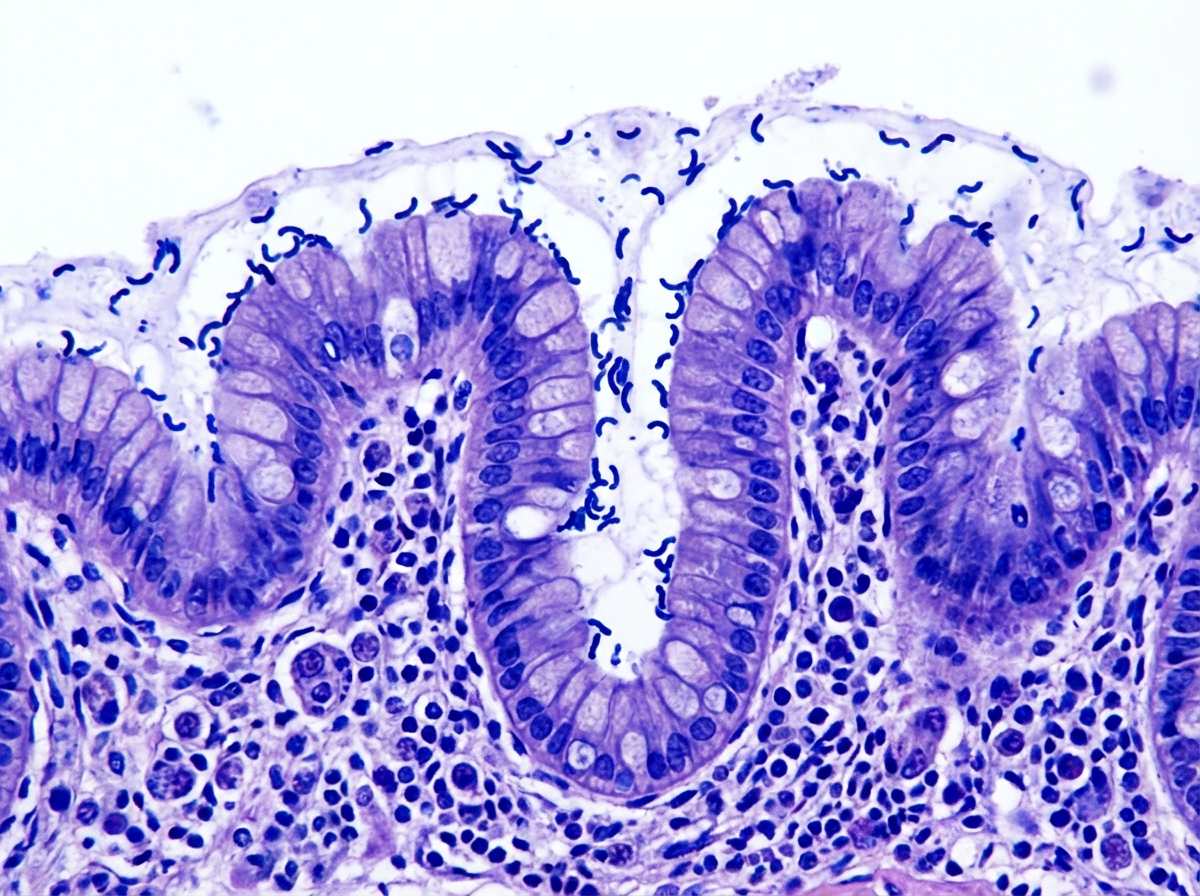
A 51-year-old man seeks evaluation from his family physician with a complaint of heartburn, which has been gradually increasing over the last 10 years. The heartburn gets worse after eating spicy foods and improves with antacids. The past medical history is benign. He is a security guard and works long hours at night. He admits to smoking 1.5 packs of cigarettes every day. Upper gastrointestinal endoscopy reveals several gastric ulcers and regions of inflammation. A biopsy is obtained, which revealed gram-negative bacteria colonized on the surface of the regenerative epithelium of the stomach, as shown in the micrograph below. Which of the following bacterial products is responsible for neutralizing the acidity of the stomach?
A 71-year-old man comes to the emergency department because of pain and swelling in his left leg that started after he cut his foot while swimming in the ocean. He has a history of alcoholic cirrhosis. His temperature is 38.3°C (101.0°F). Examination of the left foot shows a small, purulent wound with surrounding swelling and dusky redness extending to the mid-calf. There are numerous hemorrhagic blisters and the entire lower leg is exquisitely tender to light palpation. There is no crepitus. Blood cultures grow gram-negative, oxidase-positive, halophilic bacilli. Which of the following is the most likely causal organism?
A 22-year-old sexually active, otherwise healthy female presents to her primary care physician complaining of several days of dysuria, frequency, urgency, and suprapubic pain. She denies fever, flank pain, vaginal itching, or vaginal bleeding/discharge. Which organism is most likely responsible for this patient's symptoms?
A 38-year-old man complains of a persistent high fever with chills, malaise, and diffuse abdominal pain for over a week. He recently returned from a trip to India. The fever began slowly and climbed its way up to 40.0°C (104.0°F) over the last 4 days. A physical exam reveals a white-coated tongue, enlarged spleen, and rose spots on the abdomen. A bone marrow aspirate was sent for culture which revealed motile gram-negative rods. Which of the following is true about the organism and the pathophysiology of this condition?
Practice by Chapter
Neisseria species (meningitidis, gonorrhoeae)
Practice Questions
Escherichia coli
Practice Questions
Klebsiella species
Practice Questions
Proteus species
Practice Questions
Pseudomonas aeruginosa
Practice Questions
Haemophilus influenzae
Practice Questions
Bordetella pertussis
Practice Questions
Legionella pneumophila
Practice Questions
Bacteroides and anaerobic gram-negatives
Practice Questions
Helicobacter pylori
Practice Questions
Campylobacter jejuni
Practice Questions
Vibrio species
Practice Questions
ESBL and CRE pathogens
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app