
Gram-negative — MCQs

On this page
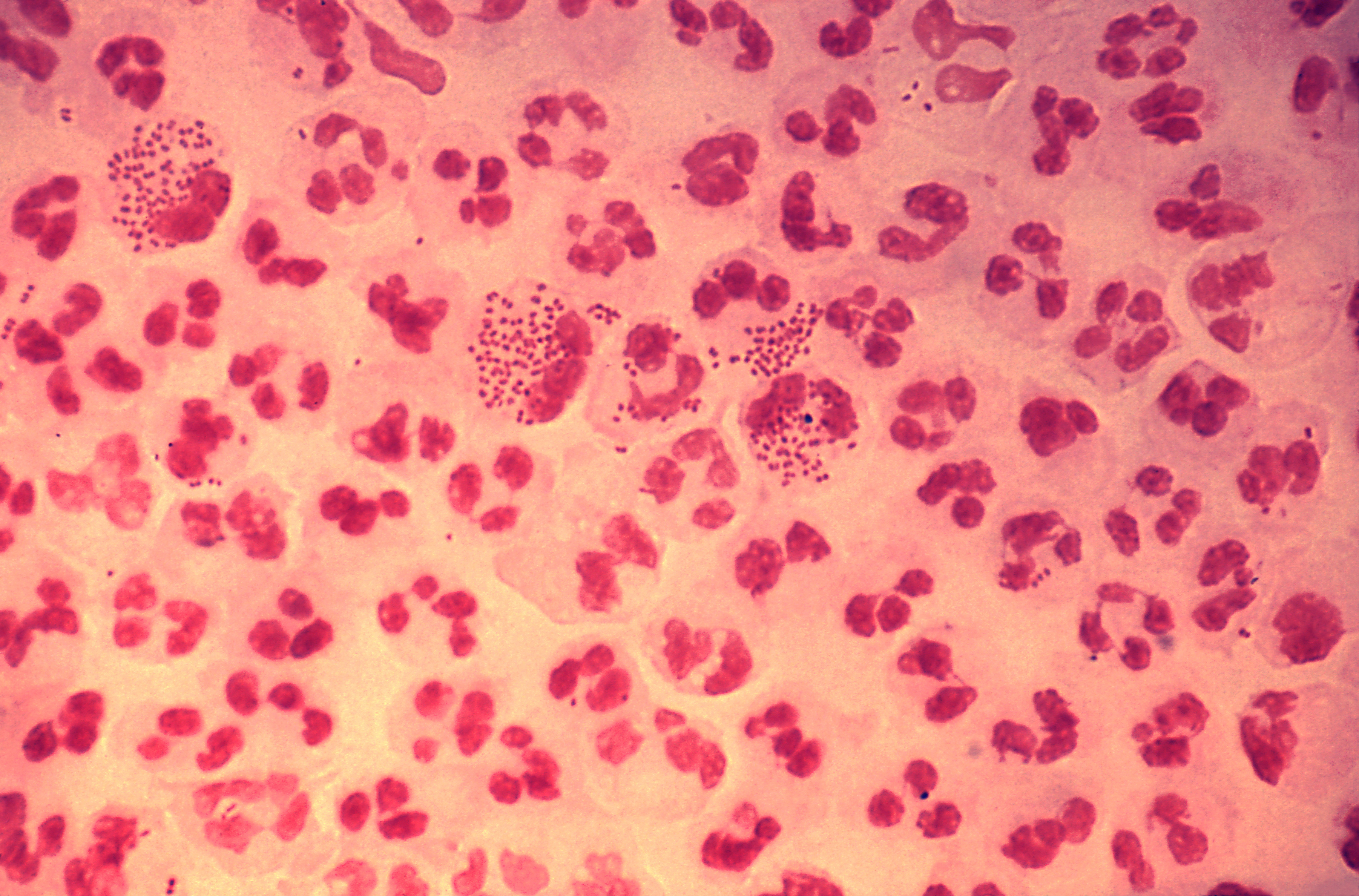
A 27-year-old woman presents to the clinic with severe pain in her left knee of 1-day duration. Physical examination reveals a red, swollen, warm, and tender left knee with a decreased range of motion. The patient affirms that she has been sexually active with several partners over the last year and that 1 of her partners has complained of dysuria and yellow urethral discharge. An arthrocentesis was performed and showed a WBC count of 60,000/µL, with 90% polymorphonuclear leukocytes. Visualization of the patient's synovial fluid is provided in the image. Which of the following is a characteristic feature of the organism causing this condition?
A 21-year-old woman comes to the physician because of a 4-day history of abdominal cramps and bloody diarrhea 5 times per day. Her symptoms began after she ate an egg sandwich from a restaurant. Her vital signs are within normal limits. Physical examination shows diffuse abdominal tenderness. Stool culture shows gram-negative rods that produce hydrogen sulfide and do not ferment lactose. Which of the following effects is most likely to occur if she receives antibiotic therapy?
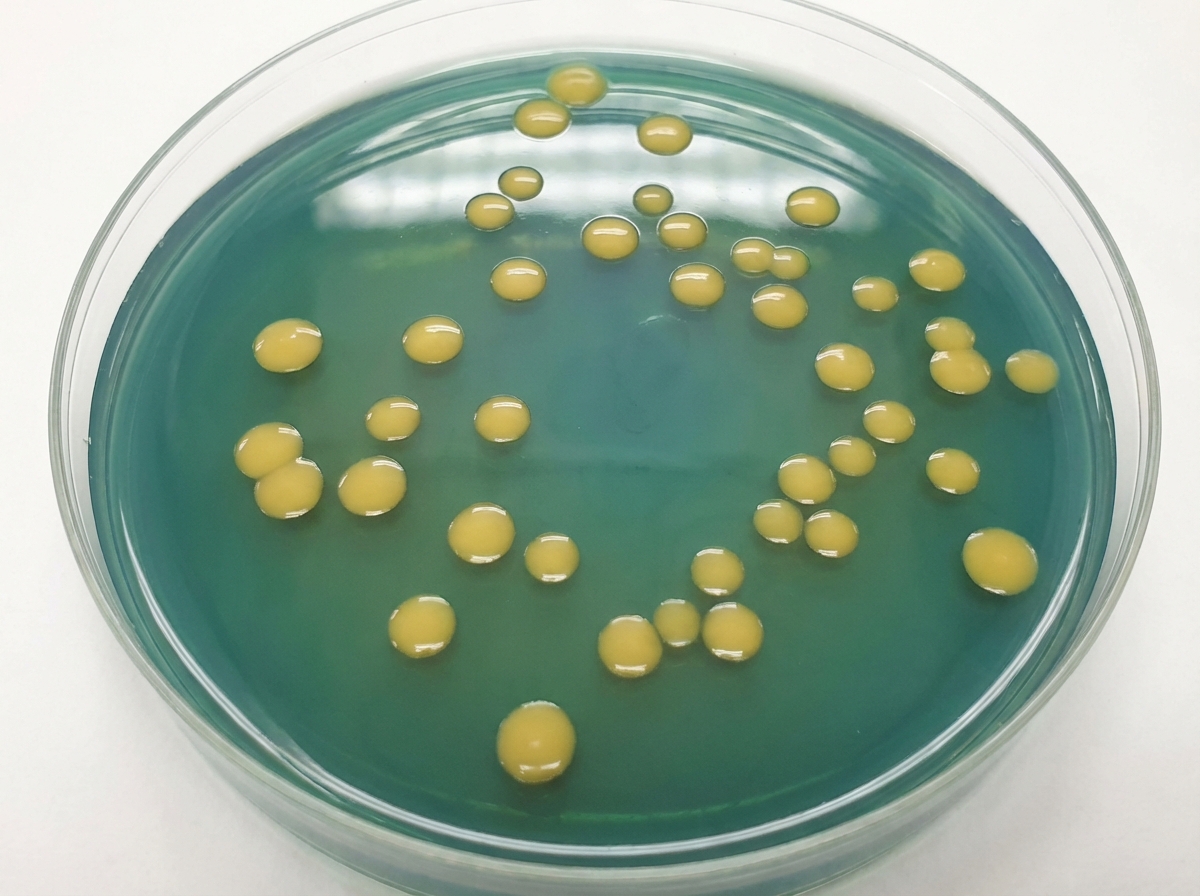
A 33-year-old man living in the United States recently consumed a meal mostly consisting of raw shellfish that his girlfriend brought on her trip to Asia. After 2 days, he experienced a sudden onset of diarrhea and vomiting with severe abdominal cramps while his girlfriend developed mild diarrhea just several hours later. The diarrhea was profuse, looked like rice water, and had a pungent fishy odor. He soon started to experience muscle cramps and weakness, together with a deep labored breathing pattern. They called an ambulance and were transported to a local hospital. Based on the symptoms and blue hue to the skin, the attending physician hospitalized the male patient, started an intravenous infusion, and sent a stool specimen to the clinical microbiology laboratory for analysis. The next day, yellow bacterial colonies were observed on thiosulfate-citrate-bile salts-sucrose agar (as shown on the image). If you were the microbiologist on call, what kind of bacterial morphology would you expect to see during microscopic evaluation of a gram-stain slide made from those bacterial colonies?
A previously healthy 26-year-old woman comes to the physician because of a 2-day history of pain with urination. She has been sexually active with two partners over the past year. She uses condoms for contraception. Vital signs are within normal limits. Physical examination shows suprapubic tenderness. Urinalysis shows neutrophils and a positive nitrite test. Urine culture grows gram-negative, oxidase-negative rods that form greenish colonies on eosin-methylene blue agar. Which of the following virulence factors of the causal organism increases the risk of infection in this patient?
A 15-year-old boy is brought to the Emergency department by ambulance from school. He started the day with some body aches and joint pain but then had several episodes of vomiting and started complaining of a terrible headache. The school nurse called for emergency services. The boy was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines and is meeting all developmental milestones. Past medical history is noncontributory. He is a good student and enjoys sports. At the hospital, his blood pressure is 120/80 mm Hg, heart rate is 105/min, respiratory rate is 21/min, and his temperature is 38.9°C (102.0°F). On physical exam, he appears drowsy with neck stiffness and sensitivity to light. Kernig’s sign is positive. An ophthalmic exam is performed followed by a lumbar puncture. An aliquot of cerebrospinal fluid is sent to microbiology. A gram stain shows gram-negative diplococci. A smear is prepared on blood agar and grows round, smooth, convex colonies with clearly defined edges. Which of the following would identify the described pathogen?
A 20-year-old woman presents for a follow-up visit with her physician. She has a history of cystic fibrosis and is currently under treatment. She has recently been struggling with recurrent bouts of cough and foul-smelling, mucopurulent sputum over the past year. Each episode lasts for about a week or so and then subsides. She does not have a fever or chills during these episodes. She has been hospitalized several times for pneumonia as a child and continues to struggle with diarrhea. Physically she appears to be underweight and in distress. Auscultation reveals reduced breath sounds on the lower lung fields with prominent rhonchi. Which of the following infectious agents is most likely associated with the recurrent symptoms this patient is experiencing?
A 65-year-old woman is brought to the emergency department by her daughter for fever and cough. She just returned from a cruise trip to the Bahamas with her family 5 days ago and reports that she has been feeling ill since then. She endorses fever, productive cough, and general malaise. Her daughter also mentions that the patient has been having some diarrhea but reports that the rest of her family has been experiencing similar symptoms. Physical examination was significant for localized crackles at the right lower lobe. Laboratory findings are as follows: Serum Na+: 130 mEq/L K+: 3.9 mEq/L Cl-: 98 mEq/L HCO3-: 27 mEq/L Mg2+: 1.8 mEq/L What findings would you expect in this patient?
An 18-year-old female college student is brought to the emergency department by ambulance for a headache and altered mental status. The patient lives with her boyfriend who is with her currently. He states she had not been feeling well for the past day and has vomited several times in the past 12 hours. Lumbar puncture is performed in the emergency room and demonstrates an increased cell count with a neutrophil predominance and gram-negative diplococci on Gram stain. The patient is started on vancomycin and ceftriaxone. Which of the following is the best next step in management?
A previously healthy 52-year-old woman comes to the physician because of a 1-week history of productive cough, fevers, and malaise. She has smoked one pack of cigarettes daily for 35 years. Her temperature is 39°C (102.2°F). Diffuse inspiratory crackles are heard bilaterally. Her leukocyte count is 14,300/mm3. Sputum analysis shows numerous polymorphonuclear leukocytes and a few squamous epithelial cells. An x-ray of the chest shows bilateral patchy consolidations. Which of the following findings on sputum culture is most consistent with this patient's respiratory symptoms?
A 15-year-old boy is admitted to the emergency department with neck stiffness, maculopapular rash, fever, and a persistent headache. A blood culture shows encapsulated gram-negative diplococci. He has had this same infection before. Which of the following proteins is likely to be deficient in this patient?
Practice by Chapter
Neisseria species (meningitidis, gonorrhoeae)
Practice Questions
Escherichia coli
Practice Questions
Klebsiella species
Practice Questions
Proteus species
Practice Questions
Pseudomonas aeruginosa
Practice Questions
Haemophilus influenzae
Practice Questions
Bordetella pertussis
Practice Questions
Legionella pneumophila
Practice Questions
Bacteroides and anaerobic gram-negatives
Practice Questions
Helicobacter pylori
Practice Questions
Campylobacter jejuni
Practice Questions
Vibrio species
Practice Questions
ESBL and CRE pathogens
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app