
Stable coronary artery disease — MCQs

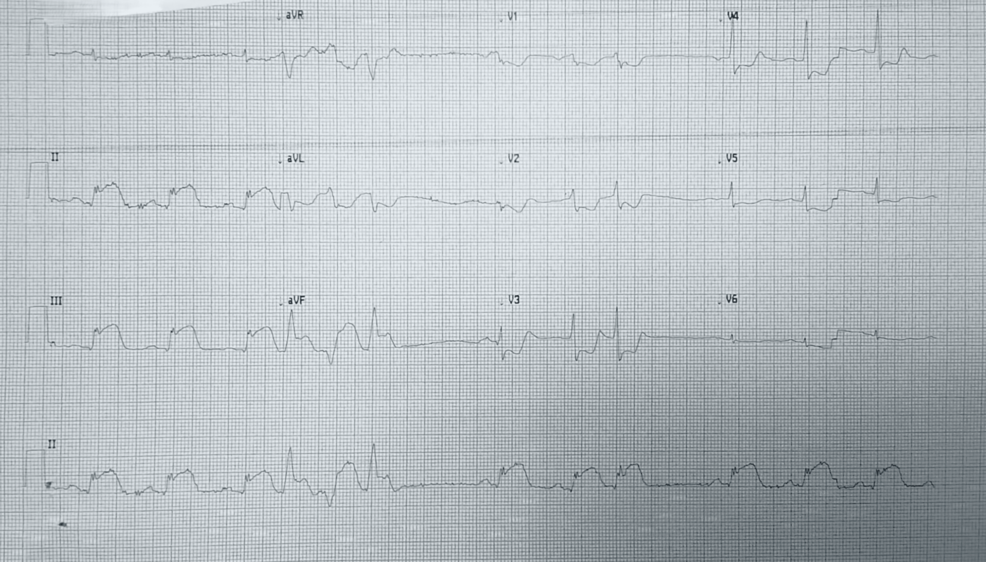
A 64-year-old man presents to the emergency department with sudden onset of chest pain and an episode of vomiting. He also complains of ongoing nausea and heavy sweating (diaphoresis). He denies having experienced such symptoms before and is quite upset. Medical history is significant for hypertension and types 2 diabetes mellitus. He currently smokes and has smoked at least half a pack daily for the last 40 years. Vitals show a blood pressure of 80/50 mm Hg, pulse of 50/min, respirations of 20/min, temperature of 37.2°C (98.9°F), and oximetry is 99% before oxygen by facemask. Except for the patient being visibly distressed and diaphoretic, the examination is unremarkable. ECG findings are shown in the picture. Where is the most likely obstruction in this patient’s cardiac blood supply?
A 73-year-old man presents to the emergency department with acute substernal chest pain that began a few hours ago. The pain is described as a "pressure" that radiates to his left arm. His past medical history is significant for hypertension and hyperlipidemia. He is on chlorthalidone for his hypertension and simvastatin for hyperlipidemia. He has a 30 pack-year history of smoking and drinks 1-2 beers on weekends. His EKG shows ST depressions in the anterior precordial leads and he is given the proper medications and sent for emergency revascularization. Seven days later, he develops dyspnea that worsens in the supine position. Bibasilar crackles are heard on pulmonary auscultation. Cardiac exam reveals a new 3/6 holosystolic murmur best heard at the apex with radiation to the axilla. What is the most likely etiology of this patient's new symptoms?
A 55-year-old man comes to the physician because of a 4-month history of episodic, pressure-like chest pain. The chest pain occurs when he is walking up stairs and improves with rest. He has hypertension and type 2 diabetes mellitus. His father died from a myocardial infarction at the age of 50 years. Current medications include hydrochlorothiazide and metformin. His pulse is 85/min, respirations are 12/min, and blood pressure is 140/90 mm Hg. Cardiac examination shows normal heart sounds without any murmurs, rubs, or gallops. An ECG shows high amplitude of the S wave in lead V3. An exercise stress test is performed but stopped after 4 minutes because the patient experiences chest pain. An ECG obtained during the stress test shows sinus tachycardia and ST-segment depressions in leads V1–V4. Which of the following is the most appropriate long-term pharmacotherapy to reduce the frequency of symptoms in this patient?
A 50-year-old man comes to the physician for his annual health maintenance examination. The patient feels well. He has a history of hypertension, for which he currently takes lisinopril. He has smoked a pack of cigarettes daily for 20 years. He drinks 5–6 beers on weekends. He is 181 cm tall (5 ft 11 in), weighs 80 kg (176.4 lbs); BMI is 24.6 kg/m2. His pulse is 75/min, blood pressure is 140/85 mm Hg, and respirations are 18/min. Physical examination is unremarkable. Laboratory studies show: Total cholesterol 263 mg/dL High-density lipoprotein cholesterol 36 mg/dL Triglycerides 180 mg/dL In addition to dietary and lifestyle modification, administration of which of the following agents is the most appropriate next step in management?
A 59-year-old man presents to his primary care provider complaining of bilateral calf cramping with walking for the past 7 months. His pain goes away when he stops walking; however, his condition affects his work as a mail carrier. His medical history is remarkable for type 2 diabetes mellitus, hyperlipidemia, and 25-pack-year smoking history. His ankle-brachial index (ABI) is found to be 0.70. The patient is diagnosed with mild to moderate peripheral artery disease. A supervised exercise program for 3 months, aspirin, and cilostazol are started. Which of the following is the best next step if the patient has no improvement?
A 59-year-old man presents to a clinic with exertional chest pain for the past several months. He says the pain is central in his chest and relieved with rest. The physical examination is unremarkable. An electrocardiogram is normal, but an exercise tolerance test revealed ST-segment depression in chest leads V1-V4. He is prescribed nitroglycerin to be taken in the first half of the day. Which of the following statements best describes the reason behind the timing of this medication?
A 39-year-old woman comes to the physician because of a 5-month history of episodic retrosternal chest pain. She currently feels well. The pain is unrelated to exercise and does not radiate. The episodes typically last less than 15 minutes and lead to feelings of anxiety; resting relieves the pain. She has not had dyspnea or cough. She has hyperlipidemia treated with simvastatin. She does not smoke, drink alcohol, or use illicit drugs. Her temperature is 37°C (98.6°F), pulse is 104/min, respirations are 17/min, and blood pressure is 124/76 mm Hg. Cardiopulmonary examination shows no abnormalities. An ECG shows sinus tachycardia. Which of the following is the most appropriate next step in the evaluation of coronary artery disease in this patient?
A 60-year-old male presents for a routine health check-up. The patient complains of reduced exercise tolerance for the past 2 years. Also, in the past year, he has noticed chest pain after climbing the stairs in his home. He has no significant past medical history or current medications. The patient reports a 45-pack-year smoking history. The vital signs include temperature 37.0°C (98.6°F), blood pressure 160/100 mm Hg, pulse 72/min, respiratory rate 15/min, and oxygen saturation 99% on room air. His body mass index (BMI) is 34 kg/m2. Physical examination is unremarkable. Laboratory studies show: Serum total cholesterol 265 mg/dL HDL 22 mg/dL LDL 130 mg/dL Triglycerides 175 mg/dL HDL: high-density lipoprotein; LDL: low-density lipoprotein Which of the following vascular pathologies is most likely present in this patient?
A 72-year-old man comes to the physician because of a 2-month history of intermittent retrosternal chest pain and tightness on exertion. He has type 2 diabetes mellitus, osteoarthritis of the right hip, and hypertension. Current medications include insulin, ibuprofen, enalapril, and hydrochlorothiazide. Vital signs are within normal limits. His troponin level is within the reference range. An ECG at rest shows a right bundle branch block and infrequent premature ventricular contractions. The patient's symptoms are reproduced during adenosine stress testing. Repeat ECG during stress testing shows new ST depression of > 1 mm in leads V2, V3, and V4. Which of the following is the most important underlying mechanism of this patient's ECG changes?
A 57-year-old man presents to his primary care provider because of chest pain for the past 3 weeks. The chest pain occurs after climbing more than 2 flight of stairs or walking for more than 10 minutes and resolves with rest. He is obese, has a history of type 2 diabetes mellitus, and has smoked 15-20 cigarettes a day for the past 25 years. His father died from a myocardial infarction at 52 years of age. Vital signs reveal a temperature of 36.7 °C (98.06°F), a blood pressure of 145/93 mm Hg, and a heart rate of 85/min. The physical examination is unremarkable. Which of the following best represents the most likely etiology of the patient’s condition?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app