
Pre-operative cardiac risk assessment — MCQs

A 70-year-old man with a recent above-the-knee amputation of the left lower extremity, due to wet gangrene secondary to refractory peripheral artery disease, presents with weakness and dizziness. He says that the symptoms began acutely 24 hours after surgery and have not improved. The amputation was complicated by substantial blood loss. He was placed on empiric antibiotic therapy with ciprofloxacin and clindamycin before the procedure, and blood and wound culture results are still pending. The medical history is significant for type 2 diabetes mellitus and hypertension. Current medications are metformin and lisinopril. The family history is significant for type 2 diabetes mellitus in both parents. Review of symptoms is significant for palpitations and a mild headache for the past 24 hours. His temperature is 38.2°C (100.8°F); blood pressure, 120/70 mm Hg (supine); pulse, 102/min; respiratory rate, 16/min; and oxygen saturation, 99% on room air. When standing, the blood pressure is 90/65 mm Hg and the pulse is 115/min. On physical examination, the patient appears pale and listless. The surgical amputation site does not show any signs of ongoing blood loss or infection. Laboratory tests and an ECG are pending. Which of the following is the next best step in management?
A patient presents with periods of severe headaches and flushing however every time they have come to the physician they have not experienced any symptoms. The only abnormal finding is a blood pressure of 175 mmHg/100 mmHg. It is determined that the optimal treatment for this patient is surgical. Prior to surgery which of the following noncompetitive inhibitors should be administered?
A 64-year-old man presents to his physician for a scheduled follow-up visit. He has chronic left-sided heart failure with systolic dysfunction. His current regular medications include captopril and digoxin, which were started after his last episode of symptomatic heart failure approximately 3 months ago. His last episode of heart failure was accompanied by atrial fibrillation, which followed an alcohol binge over a weekend. Since then he stopped drinking. He reports that he has no current symptoms at rest and is able to perform regular physical exercise without limitation. On physical examination, mild bipedal edema is noted. The physician suggested to him that he should discontinue digoxin and continue captopril and scheduled him for the next follow-up visit. Which of the following statements best justifies the suggestion made by the physician?
A 62-year-old man comes to the physician in May for a routine health maintenance examination. He feels well. He underwent a right inguinal hernia repair 6 months ago. He has hypertension and type 2 diabetes mellitus. There is no family history of serious illness. Current medications include metformin, sitagliptin, enalapril, and metoprolol. He received the zoster vaccine 1 year ago. He received the PPSV23 vaccine 4 years ago. His last colonoscopy was 7 years ago and was normal. He smoked a pack of cigarettes a day for 20 years but quit 17 years ago. He drinks two to three alcoholic beverages on weekends. He is allergic to amoxicillin. He is scheduled to visit Australia and New Zealand in 2 weeks to celebrate his 25th wedding anniversary. He appears healthy. Vital signs are within normal limits. An S4 is heard at the apex. The remainder of the examination shows no abnormalities. Which of the following is the most appropriate recommendation at this time?
A 50-year-old woman comes to the physician for a routine health maintenance examination. She has no personal or family history of serious illness. She smoked one pack of cigarettes daily for 5 years during her 20s. Her pulse is 70/min, and blood pressure is 120/78 mm Hg. Serum lipid studies and glucose concentration are within the reference ranges. Which of the following health maintenance recommendations is most appropriate at this time?
An 83-year-old male presents with dyspnea, orthopnea, and a chest radiograph demonstrating pulmonary edema. A diagnosis of congestive heart failure is considered. The following clinical measurements are obtained: 100 bpm heart rate, 0.2 mL O2/mL systemic blood arterial oxygen content, 0.1 mL O2/mL pulmonary arterial oxygen content, and 400 mL O2/min oxygen consumption. Using the above information, which of the following values represents this patient's cardiac stroke volume?
A 41-year-old man presents to his primary care provider because of chest pain with activity for the past 6 months. Past medical history is significant for appendectomy at age 12 and hypertension, and diabetes mellitus type 2 that is poorly controlled. He takes metformin and lisinopril but admits that he is bad at remembering to take them everyday. His father had a heart attack at 41 and 2 stents were placed in his heart. His mother is healthy. He drinks alcohol occasionally and smokes a half of a pack of cigarettes a day. He is a sales executive and describes his work as stressful. Today, the blood pressure is 142/85 and the body mass index (BMI) is 28.5 kg/m2. A coronary angiogram shows > 75% narrowing of the left anterior descending coronary artery. Which of the following is most significant in this patient?
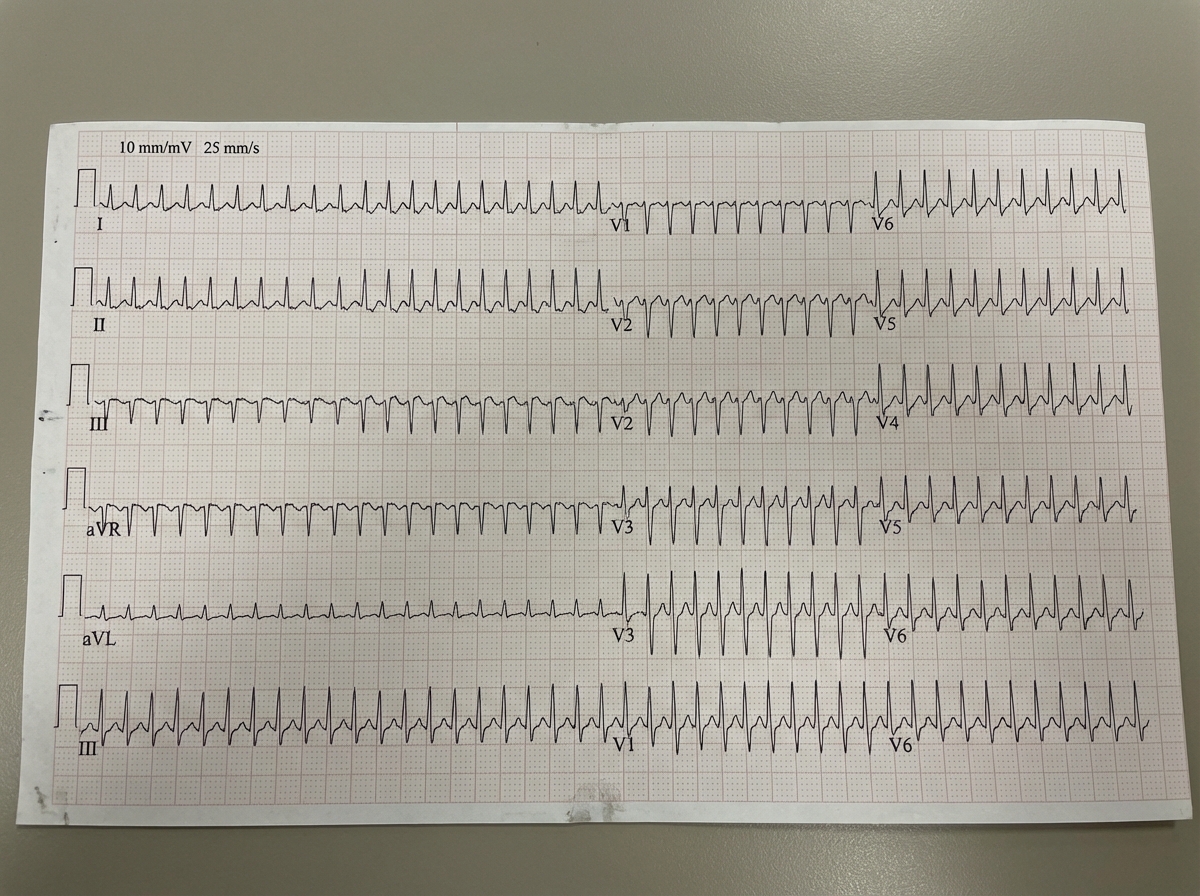
A 43-year-old man comes to the emergency room complaining of chest discomfort. He describes the feeling as "tightness," and also reports weakness and palpitations for the past hour. He denies shortness of breath, diaphoresis, or lightheadedness. He has no significant past medical history, and does not smoke, drink, or use illicit drugs. His father had a myocardial infarction at age 72. He is afebrile, heart rate is 125 bpm, and his blood pressure is 120/76. He is alert and oriented to person, place, and time. His electrocardiogram is shown below. Which of the following tests should be ordered in the initial work-up of this patient's condition?
A 66-year-old female with hypertension and a recent history of acute ST-elevation myocardial infarction (STEMI) 6 days previous, treated with percutaneous transluminal angioplasty (PTA), presents with sudden onset chest pain, shortness of breath, diaphoresis, and syncope. Vitals are temperature 37°C (98.6°F), blood pressure 80/50 mm Hg, pulse 125/min, respirations 12/min, and oxygen saturation 92% on room air. On physical examination, the patient is pale and unresponsive. Cardiac exam reveals tachycardia and a pronounced holosystolic murmur loudest at the apex and radiates to the back. Lungs are clear to auscultation. Chest X-ray shows cardiomegaly with clear lung fields. ECG is significant for ST elevations in the precordial leads (V2-V4) and low-voltage QRS complexes. Emergency transthoracic echocardiography shows a left ventricular wall motion abnormality along with a significant pericardial effusion. The patient is intubated, and aggressive fluid resuscitation is initiated. What is the next best step in management?
A 39-year-old woman comes to the physician because of a 5-month history of episodic retrosternal chest pain. She currently feels well. The pain is unrelated to exercise and does not radiate. The episodes typically last less than 15 minutes and lead to feelings of anxiety; resting relieves the pain. She has not had dyspnea or cough. She has hyperlipidemia treated with simvastatin. She does not smoke, drink alcohol, or use illicit drugs. Her temperature is 37°C (98.6°F), pulse is 104/min, respirations are 17/min, and blood pressure is 124/76 mm Hg. Cardiopulmonary examination shows no abnormalities. An ECG shows sinus tachycardia. Which of the following is the most appropriate next step in the evaluation of coronary artery disease in this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app