
Peripheral arterial disease — MCQs

A 70-year-old man comes to the physician for the evaluation of pain, cramps, and tingling in his lower extremities over the past 6 months. The patient reports that the symptoms worsen with walking more than two blocks and are completely relieved by rest. Over the past 3 months, his symptoms have not improved despite his participating in supervised exercise therapy. He has type 2 diabetes mellitus. He had smoked one pack of cigarettes daily for the past 50 years, but quit 3 months ago. He does not drink alcohol. His current medications include metformin, atorvastatin, and aspirin. Examination shows loss of hair and decreased skin temperature in the lower legs. Femoral pulses are palpable; pedal pulses are absent. Which of the following is the most appropriate treatment for this patient?
A 67-year-old man comes to the office due to pain in the lower part of his calves on his afternoon walk to get the mail. The pain is relieved by rest. It started slowly about 6 months ago and has become more painful over time. He has a history of hypertension, hyperlipidemia, diabetes mellitus, and a 20-pack-year smoking history. Medications include hydrochlorothiazide, atorvastatin, metformin, and a multivitamin that he takes daily. The patient quit smoking 2 years ago and only drinks socially. Today, his blood pressure is 145/90 mm Hg, pulse is 75/min, respiratory rate is 17/min, and temperature is 37.6°C (99.6°F). On physical exam, he appears mildly obese and healthy. His heart has a regular rate and rhythm, and his lungs are clear to auscultation bilaterally. Examination of the legs shows atrophic changes and diminished pedal pulses. A measure of his ankle brachial index (ABI) is 0.89. Which of the following is the most appropriate initial treatment?
A 53-year-old Asian woman comes to the physician because of a 2-month history of severe pain in her right leg while walking. She used to be able to walk a half-mile (800-m) to the grocery store but has been unable to walk 200 meters without stopping because of the pain over the past month. She can continue to walk after a break of around 5 minutes. She has hypertension, atrial fibrillation, and type 2 diabetes mellitus. She has smoked one pack of cigarettes daily for the past 32 years. Current medications include metformin, enalapril, aspirin, and warfarin. Vital signs are within normal limits. Examination shows an irregularly irregular pulse. The right lower extremity is cooler than the left lower extremity. The skin over the right leg appears shiny and dry. Femoral pulses are palpated bilaterally; pedal pulses are diminished on the right side. Which of the following is the most appropriate next step in management?
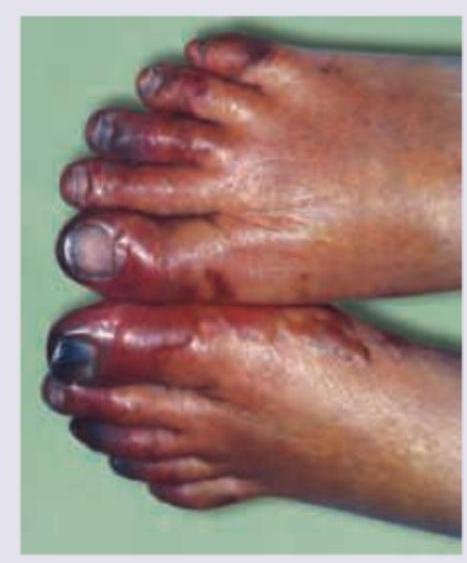
A 75-year-old man presents to the emergency department because of pain in his left thigh and left calf for the past 3 months. The pain occurs at rest, worsens with walking, and is slightly improved by hanging his foot off the bed. He has had hypertension for 25 years and type 2 diabetes mellitus for 30 years. He has smoked 30–40 cigarettes per day for the past 45 years. On examination, the femoral, popliteal, and dorsalis pedis pulses are diminished, but detectable on both sides. The patient’s foot is shown in the image. Which of the following is the most likely diagnosis?

A 58-year-old man comes to the physician because of a 3-month history of intermittent pain in his right calf that occurs after walking up more than 2 flights of stairs. He reports that the pain is associated with a tingling sensation and lasts for about 10 minutes. He is otherwise healthy. He has smoked 2 packs of cigarettes daily for 30 years and drinks 1 alcoholic beverage daily. He currently takes no medications. His pulse is 78/min, and blood pressure is 180/110 mm Hg. Physical examination shows yellow plaques below the lower eyelids bilaterally, loss of hair on the distal third of the right leg, and brittle toenails on the right foot. Femoral pulses are palpable bilaterally; right popliteal and pedal pulses are absent. Which of the following is the most appropriate management to prevent future morbidity and mortality of this patient's condition?
A 75-year-old man presents to the emergency department because of pain in his left thigh and left calf for the past 3 months. The pain occurs at rest, increases with walking, and is mildly improved by hanging the foot off the bed. He has had hypertension for 25 years and type 2 diabetes mellitus for 30 years. He has smoked 30–40 cigarettes per day for the past 45 years. On examination, femoral, popliteal, and dorsalis pedis pulses are faint on both sides. The patient’s foot is shown in the image. Resting ankle-brachial index (ABI) is found to be 0.30. Antiplatelet therapy and aggressive risk factors modifications are initiated. Which of the following is the best next step for this patient?
A 66-year-old woman presents to the emergency department with lower extremity pain. She reports that she has had worsening pain in her left calf over the past year while walking. The pain improves with rest, but the patient notes that she now has to stop walking more frequently than in the past to relieve the pain. The patient’s past medical history is otherwise notable for hypertension and coronary artery disease. Her home medications include hydrochlorothiazide and lisinopril. Her family history is significant for diabetes mellitus in her father. On physical exam, her left lower extremity is slightly cool to the touch with palpable distal pulses. The skin of the left lower extremity appears smooth and shiny below the mid-calf. Laboratory testing is performed and reveals the following: Serum: High-density lipoprotein (HDL): 60 mg/dL Low-density lipoprotein (LDL): 96 mg/dL Triglycerides: 140 mg/dL This patient should be started on which of the following medication regimens?
A 58-year-old man presents to the emergency department with severe right leg pain accompanied by tingling and weakness. His condition started suddenly 3 hours ago when he was watching a movie. His medical history is remarkable for type 2 diabetes mellitus and hypertension. He has been smoking 20–30 cigarettes per day for the past 35 years. His vital signs include a blood pressure of 149/85 mm Hg, a temperature of 36.9°C (98.4°F), and an irregular pulse of 96/min. On physical examination, his right popliteal and posterior tibial pulses are absent. His right leg is pale and cold. Which of the following is the most likely diagnosis?
A 65-year-old man comes to the physician because of a 10-month history of crampy left lower extremity pain that is exacerbated by walking and relieved by rest. The pain is especially severe when he walks on an incline. He has a 20-year history of type 2 diabetes mellitus, for which he takes metformin. He has smoked 1 pack of cigarettes daily for 40 years. His blood pressure is 140/92 mm Hg. Physical examination shows dry and hairless skin over the left foot. Which of the following is the most likely underlying cause of this patient's symptoms?
A 49-year-old man comes to the physician because of increasing difficulty achieving an erection for 6 months. During this period, he has had to reduce his hours as a construction worker because of pain in his lower back and thighs and a progressive lower limb weakness when walking for longer distances. His pain resolves after resting for a few minutes, but it recurs when he returns to work. He also reports that his pain is improved by standing still. He is sexually active with 4 female partners and uses condoms irregularly. His father has coronary artery disease and his mother died of a ruptured intracranial aneurysm at the age of 53 years. He has smoked one pack of cigarettes daily for 35 years. He has recently taken sildenafil, given to him by a friend, with no improvement in his symptoms. His only other medication is ibuprofen as needed for back pain. His last visit to a physician was 25 years ago. He is 172.5 cm (5 ft 8 in) tall and weighs 102 kg (225 lb); BMI is 34.2 kg/m2. His temperature is 36.9°C (98.4°F), pulse is 76/min, and blood pressure is 169/98 mm Hg. A complete blood count and serum concentrations of electrolytes, urea nitrogen, and creatinine are within the reference ranges. His hemoglobin A1c is 6.2%. Which of the following is the most likely finding on physical examination?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app