
Pericardial diseases — MCQs

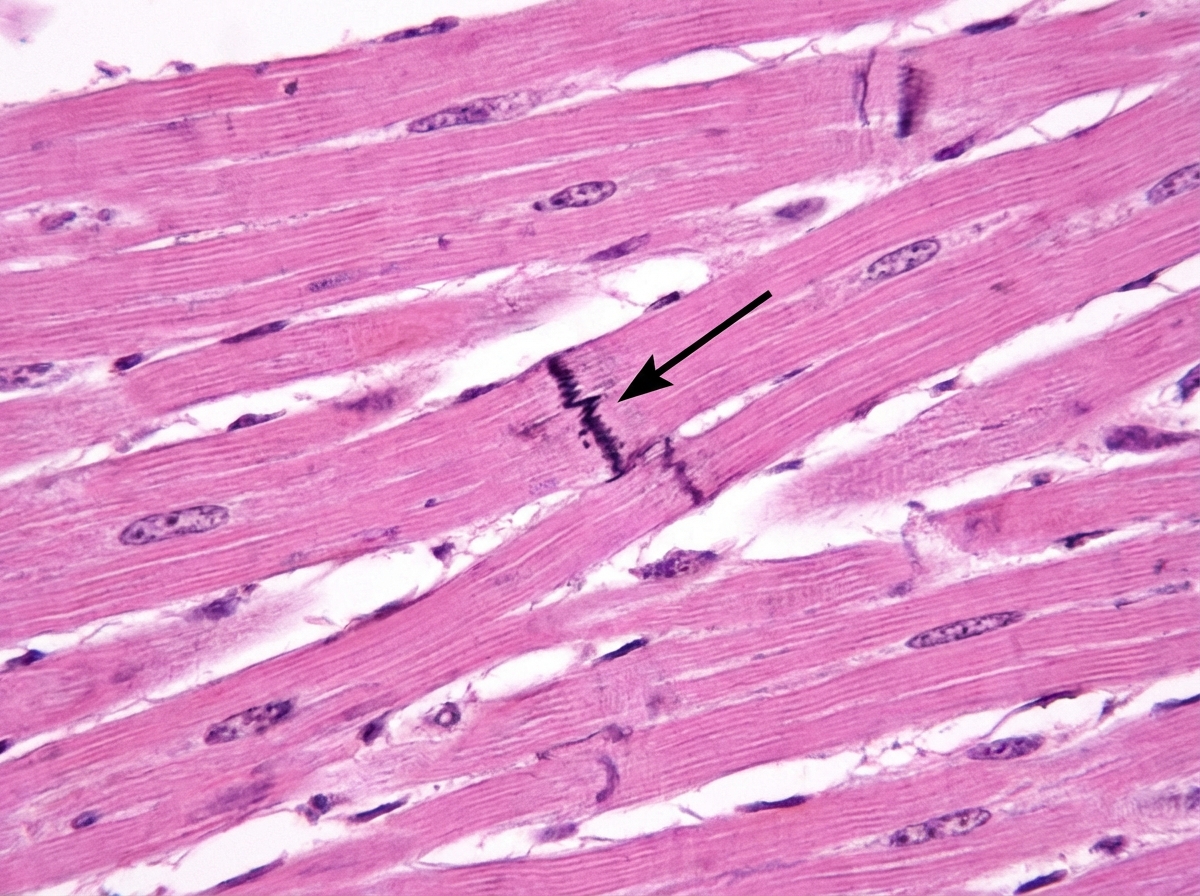
Cardiac muscle serves many necessary functions, leading to a specific structure that serves these functions. The structure highlighted is an important histology component of cardiac muscle. What would be the outcome if this structure diffusely failed to function?
On the 3rd day post-anteroseptal myocardial infarction (MI), a 55-year-old man who was admitted to the intensive care unit is undergoing an examination by his physician. The patient complains of new-onset precordial pain which radiates to the trapezius ridge. The nurse informs the physician that his temperature was 37.7°C (99.9°F) 2 hours ago. On physical examination, the vital signs are stable, but the physician notes the presence of a triphasic pericardial friction rub on auscultation. A bedside electrocardiogram shows persistent positive T waves in leads V1–V3 and an ST segment: T wave ratio of 0.27 in lead V6. Which of the following is the drug of choice to treat the condition the patient has developed?
A 16-year-old boy with a history of severe, persistent asthma presents to the emergency department with severe shortness of breath and cough. He states that he was outside playing basketball with his friends, forgot to take his inhaler, and began to have severe difficulty breathing. On exam, he is in clear respiratory distress with decreased air movement throughout all lung fields. He is immediately treated with beta-agonists which markedly improve his symptoms. Prior to treatment, which of the following was most likely observed in this patient?
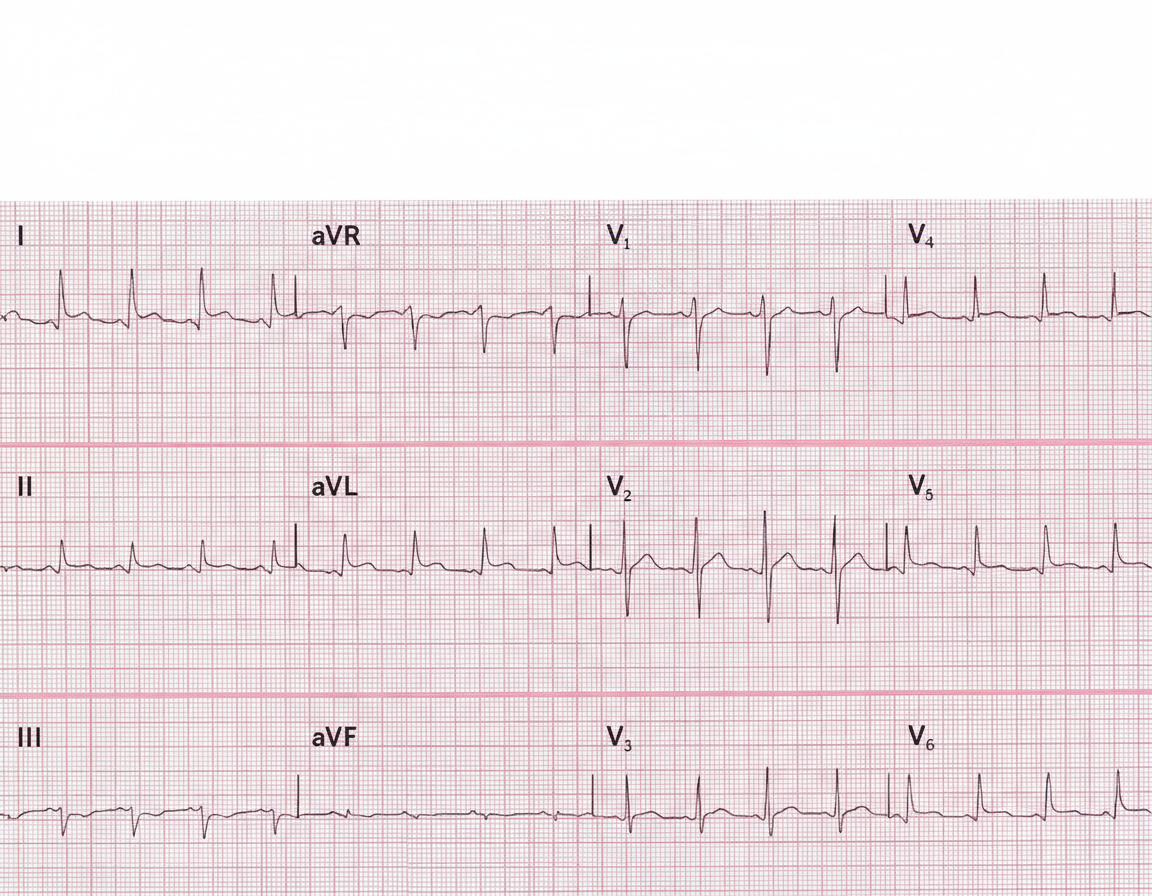
A 29-year-old man presents to the emergency department with a sharp pain in the center of his chest. The pain is knife-like and constant. Sitting alleviates the pain and lying supine aggravates it. He denies the use of nicotine, alcohol or illicit drugs. Vital signs include: temperature 37.0°C (98.6°F), blood pressure 135/92 mm Hg, and pulse 97/min. On examination, a friction rub is heard at the left sternal border while the patient is leaning forward. His ECG is shown in the image. Which of the following can prevent recurrence of this patient’s condition?
A 41-year-old woman presents to the emergency room with chest pain. She has had progressive substernal chest pain accompanied by weakness and mild shortness of breath for the past 2 hours. Her past medical history is notable for poorly controlled systemic lupus erythematosus (SLE), Sjogren syndrome, and interstitial lung disease. She was hospitalized last year with pericarditis presumed to be from SLE. Her temperature is 98.6°F (37°C), blood pressure is 106/56 mmHg, pulse is 132/min, and respirations are 26/min. On exam, the skin overlying the internal jugular vein fills at 9 cm above the sternal angle and distant heart sounds are appreciated. There is no friction rub. She is given 1000cc of intravenous fluids with no appreciable change in her blood pressure. An electrocardiogram in this patient would most likely reveal which of the following findings?
An 80-year-old man presents to the emergency department because of gnawing substernal chest pain that started an hour ago and radiates to his neck and left jaw. A 12-lead ECG is obtained and shows ST-segment elevation with newly developing Q waves. He is admitted for treatment. 4 days after hospitalization he suddenly develops altered mental status, and his blood pressure falls from 115/75 mm Hg to 80/40 mm Hg. Physical examination shows jugular venous distention, pulsus paradoxus, and distant heart sounds. What is the most likely cause of this patient's condition?
A 54-year-old woman presents to the emergency ward with a chief complaint of chest pain. The pain is sharp and present in the anterior part of the chest. There is no radiation of the pain; however, the intensity is decreased while sitting and leaning forward. There is no associated shortness of breath. Vital signs are the following: blood pressure is 132/84 mm Hg; pulse rate is 82/min, rhythmic, and regular. Lungs are clear on auscultation and cardiovascular examination demonstrates scratchy and squeaking sounds at the left sternal border. Kussmaul sign is positive and ECG shows new widespread ST segment elevation and PR depression. The most likely cause for these findings in this patient is?
A 74-year-old man comes to the physician for a 6-month history of progressively worsening fatigue and shortness of breath on exertion. He immigrated to the United States 35 years ago from India. His pulse is 89/min and blood pressure is 145/60 mm Hg. Crackles are heard at the lung bases. Cardiac examination shows a grade 3/6 early diastolic murmur loudest at the third left intercostal space. Further evaluation of this patient is most likely to show which of the following?
A 72-year-old man presents to the emergency department because of difficulty breathing and sharp chest pain. The chest pain increases in intensity with lying down, and it radiates to the scapular ridge. Approximately 3 weeks ago, he had an anterior ST-elevation myocardial infarction, which was treated with intravenous alteplase. He was discharged home in a stable condition. Current vital signs include a temperature of 38.1 (100.5°F), blood pressure of 131/91 mm Hg, and pulse of 99/min. On examination, heart sounds are distant and a scratching sound is heard on the left sternal border. ECG reveals widespread concave ST elevations in the precordial leads and PR depressions in leads V2-V6. Which of the following is the most likely cause of this patient condition?
A 77-year-old woman presents to her physician because of fatigue and progressive dyspnea despite receiving optimal treatment for heart failure. Her medical history is positive for heart failure, active tuberculosis, and chronic renal failure, for which she has been in long-term hemodialysis (13 years). The woman currently takes rifampin and isoniazid. Her physical exam shows the presence of hepatomegaly and jugular venous distention that fails to subside on inspiration (Kussmaul's sign) and an impalpable apical impulse. Her pulse is 122/min, respiratory rate 16/min, temperature 36.0°C (97.4°F), and blood pressure 120/60 mm Hg. Her cardiac monitor shows a prominent y descent in her jugular venous pulse. A cardiac ultrasound shows pericardial calcifications and small tubular-shaped ventricles. Which of the following is the most likely cause of this patient's current condition?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app