
Cardiac tumors — MCQs

A 68-year-old man comes to the emergency department because of a 1-week history of difficulty breathing. He has had recurrent palpitations over the past 2 years. During this time, he has also had several episodes of anxiety despite no change in his daily life. He has occasional sharp chest pain localized to the left upper sternal border. He has no abdominal pain or leg swelling. Two years ago, he had streptococcal pharyngitis, which was promptly treated with a 10-day course of penicillin. He has never traveled outside of the country. His temperature is 36.5°C (97.7°F), pulse is 82/min, and blood pressure is 140/85 mm Hg. Physical examination shows a 3/6 holosystolic murmur that is loudest at the apex and radiates to the axilla with a mid-systolic click. Bilateral fine crackles are heard on lung auscultation. Which of the following is the most likely cause of this patient's symptoms?
A 38-year-old woman comes to the physician because of a 10-month history of nonbloody diarrhea and recurrent episodes of flushing and wheezing. She does not take any medications. Physical examination shows a hyperpigmented rash around the base of her neck. Cardiac examination shows a grade 4/6, holosystolic murmur in the 5th intercostal space at the left midclavicular line. Echocardiography shows left-sided endocardial and valvular fibrosis with moderate mitral regurgitation; there are no septal defects or right-sided valvular defects. Urinalysis shows increased 5-hydroxyindoleacetic acid concentration. Further evaluation of this patient is most likely to show which of the following findings?
A 48-year-old woman comes to the physician because of progressively worsening dyspnea on exertion and fatigue for the past 2 months. She had Hodgkin lymphoma as an adolescent, which was treated successfully with chemotherapy and radiation. Her father died from complications related to amyloidosis. She does not smoke or drink alcohol. Her temperature is 36.7°C (98°F), pulse is 124/min, respirations are 20/min, and blood pressure is 98/60 mm Hg. Cardiac examination shows no murmurs. Coarse crackles are heard at the lung bases bilaterally. An ECG shows an irregularly irregular rhythm with absent P waves. An x-ray of the chest shows globular enlargement of the cardiac shadow with prominent hila and bilateral fluffy infiltrates. Transthoracic echocardiography shows a dilated left ventricle with an ejection fraction of 40%. Which of the following is the most likely cause of this patient's condition?
A 62-year-old woman presents to the emergency department with a 2-hour history of sharp chest pain. She says that the pain is worse when she inhales and is relieved by sitting up and leaning forward. Her past medical history is significant for rheumatoid arthritis, myocardial infarction status post coronary artery bypass graft, and radiation for breast cancer 20 years ago. Physical exam reveals a rubbing sound upon cardiac auscultation as well as increased jugular venous distention on inspiration. Pericardiocentesis is performed revealing grossly bloody fluid. Which of the following is most specifically associated with this patient's presentation?
A previously healthy 20-year-old man is brought to the emergency department 15 minutes after collapsing while playing basketball. He has no history of serious illness. On arrival, there is no palpable pulse or respiratory effort observed. He is declared dead. The family agrees to an autopsy. Cardiac workup prior to this patient's death would most likely have shown which of the following findings?
A 53-year-old woman comes to the physician because of increasing shortness of breath on exertion for 5 months. She reports that she can not climb more than 2 flights of stairs and she is no longer able to run her errands as usual. One year ago, she was diagnosed with triple-negative breast cancer. She underwent a right-sided modified radical mastectomy and adjuvant chemotherapy. Cardiac examination shows a laterally displaced point of maximal impulse. Coarse inspiratory crackles are heard in both lower lung fields. Echocardiography shows a left ventricular ejection fraction of 30%. The physician informs the patient that her symptoms are most likely due to an adverse effect of her chemotherapy. The drug most likely responsible for the patient's current symptoms belongs to which of the following groups of agents?
A 52-year-old woman comes to the physician because of a 1-month history of mild fever, fatigue, and shortness of breath. She has no history of serious medical illness and takes no medications. Cardiopulmonary examination shows a mid-diastolic plopping sound heard best at the apex and bilateral rales at the base of the lungs. Echocardiography shows a pedunculated, heterogeneous mass in the left atrium. A biopsy of the mass shows clusters of mesenchymal cells surrounded by gelatinous material. Further evaluation of this patient is most likely to show which of the following?
A 69-year-old man is scheduled to undergo radical retropubic prostatectomy for prostate cancer in 2 weeks. He had a myocardial infarction at the age of 54 years. He has a history of GERD, unstable angina, hyperlipidemia, and severe osteoarthritis in the left hip. He is unable to climb up stairs or walk fast because of pain in his left hip. He had smoked one pack of cigarettes daily for 30 years but quit 25 years ago. He drinks one glass of wine daily. Current medications include aspirin, metoprolol, lisinopril, rosuvastatin, omeprazole, and ibuprofen as needed. His temperature is 36.4°C (97.5°F), pulse is 90/min, and blood pressure is 136/88 mm Hg. Physical examination shows no abnormalities. A 12-lead ECG shows Q waves and inverted T waves in leads II, III, and aVF. His B-type natriuretic protein is 84 pg/mL (N < 125). Which of the following is the most appropriate next step in management to assess this patient's perioperative cardiac risk?
A 38-year-old woman is referred to a cardiologist for evaluation of syncope. Over the past year she has experienced 2 syncopal events. The first event occurred while she was standing, and the second when she laid down on her side. She denies bowel or bladder incontinence during the episodes or palpitations. However, she reports the presence of a low-grade fever over the past 3 months and a recent visit to the emergency department for a transient ischemic attack. She has a history of intravenous drug use but reports not having used in over 5 years. Temperature is 100.0°F (37.8°C), blood pressure is 115/72 mmHg, pulse is 90/min, and respirations are 20/min and regular. A detailed neurologic examination reveals no focal deficits. Cardiac auscultation demonstrates a diastolic "plop" at the cardiac apex. Which of the following findings will most likely be demonstrated on transthoracic echocardiography?
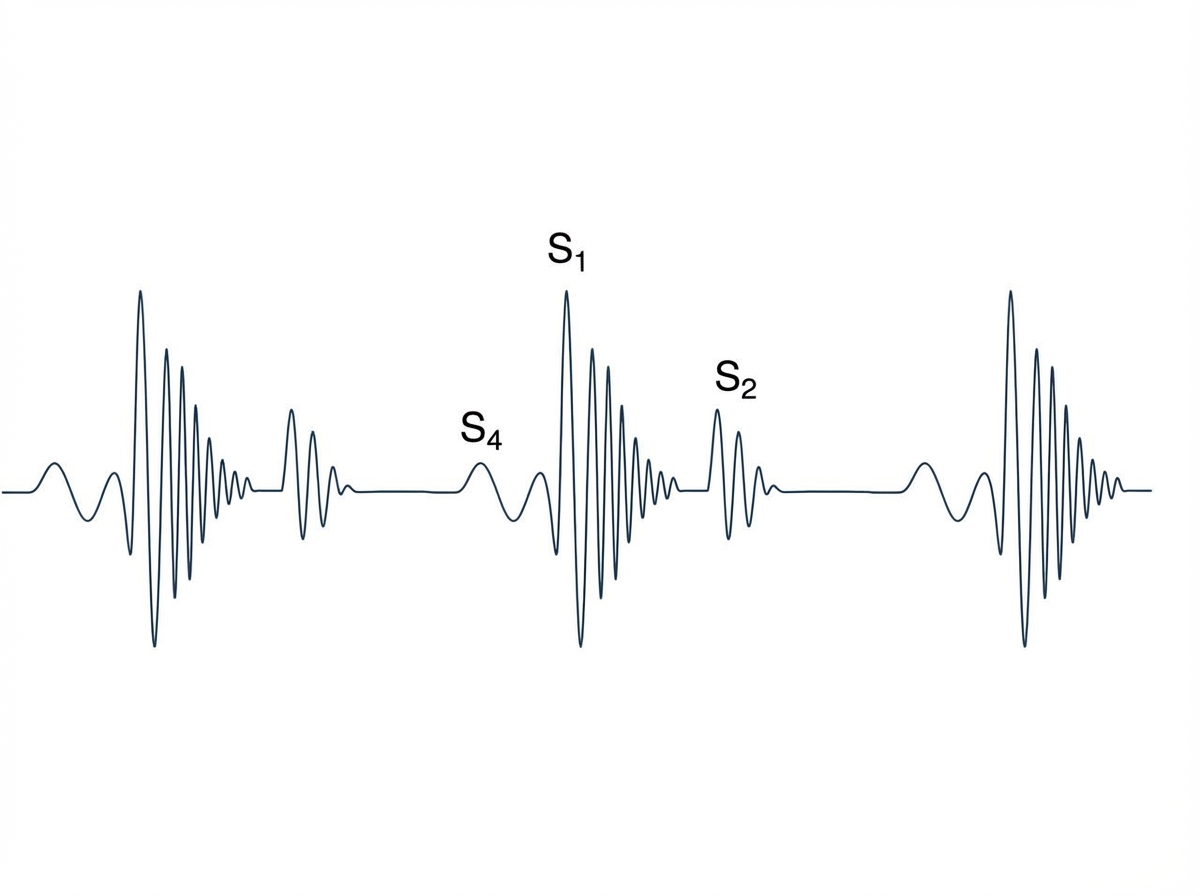
A 65-year-old man with hypertension comes to the physician for a routine health maintenance examination. Current medications include atenolol, lisinopril, and atorvastatin. His pulse is 86/min, respirations are 18/min, and blood pressure is 145/95 mm Hg. Cardiac examination is shown. Which of the following is the most likely cause of this physical examination finding?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app