
Aortic diseases — MCQs

A 62-year-old man is brought to the emergency department with a sudden onset of severe chest pain, that he describes as tearing. The pain started 90 minutes back and is now referring to the upper back. There is a history of essential hypertension for the past 17 years. The patient has smoked 20–30 cigarettes daily for the past 27 years. Vital signs reveal: temperature 36.8°C (98.2°F), heart rate 105/min, and blood pressure 192/91 mm Hg in the right arm and 159/81 mm Hg in the left arm. Pulses are absent in the right leg and diminished in the left. ECG shows sinus tachycardia, and chest X-ray shows a widened mediastinum. Transthoracic echocardiography shows an intimal flap arising from the ascending aorta and extended to the left subclavian artery. Intravenous morphine sulfate is started. Which of the following is the best next step in the management of this patient condition?
A 24-year-old man presents with a complaint of breathlessness while jogging. He says that he recently started marathon training. He does not have any family history of asthma nor has any allergies. He currently takes no medication. The blood pressure is 120/80 mm Hg, and the heart rate is 67/min. With each heartbeat, he experiences pounding in his chest, and his head bobs. On physical examination, he has long fingers, funnel chest, and disproportionate body proportions with a decreased upper-to-lower segment ratio. On auscultation over the 2nd right intercostal space, an early diastolic murmur is heard, and 3rd and 4th heart sounds are heard. Echocardiography shows aortic root dilatation. The patient is scheduled for surgery. Which of the following is associated with this patient's condition?
A 75-year-old Caucasian man presents to the emergency department with abdominal pain. The patient states he was at home eating dinner when he began to experience severe abdominal pain. The patient has a past medical history of diabetes, hypertension, and atherosclerosis. He lives at home alone, smokes cigarettes, and drinks 1 to 2 alcoholic drinks per day. The patient is given IV morphine and an ultrasound is obtained demonstrating a dilated abdominal aorta. The patient states that his father died of a similar finding and is concerned about his prognosis. Which of the following is the greatest risk factor for this patient's presentation?
A 32-year-old woman who recently emigrated to the USA from Japan comes to the physician because of a 3-month history of night sweats, malaise, and joint pain. During this time, she has also had a 6-kg (13-lb) weight loss. Physical examination shows weak brachial and radial pulses. There are tender subcutaneous nodules on both legs. Carotid bruits are heard on auscultation bilaterally. Laboratory studies show an erythrocyte sedimentation rate of 96 mm/h. A CT scan of the chest shows thickening and narrowing of the aortic arch. Microscopic examination of the aortic arch is most likely to show which of the following findings?
A 65-year-old man with hypertension and type 2 diabetes mellitus is brought to the emergency department 20 minutes after the onset of severe anterior chest pain and shortness of breath. He has smoked one pack of cigarettes daily for 30 years. He appears distressed. His pulse is 116/min, respirations are 22/min, and blood pressure is 156/88 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 98%. A grade 3/6, high-pitched, blowing, diastolic murmur is heard over the right upper sternal border. Which of the following is the most likely cause of this patient's symptoms?
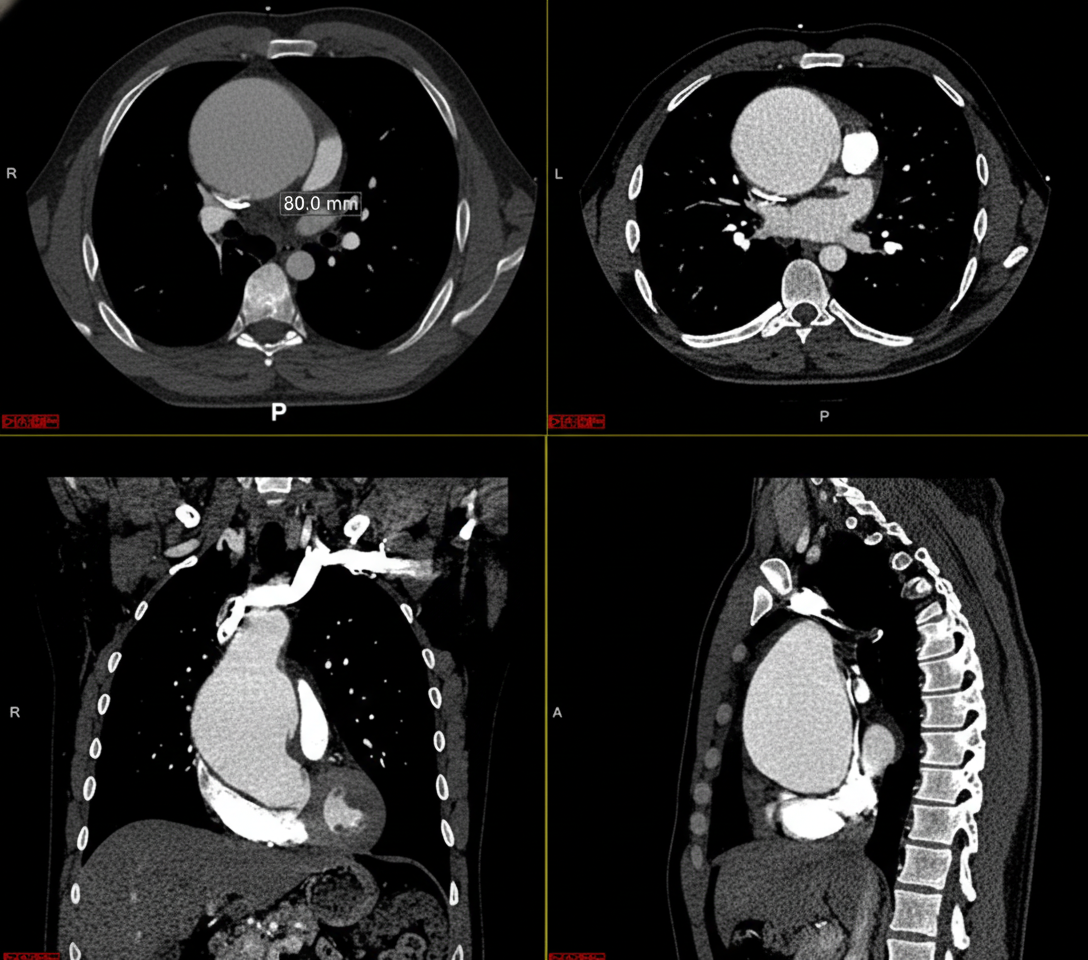
A previously healthy 32-year-old man comes to the physician because of a 1-week history of upper back pain, dyspnea, and a sensation of pressure in his chest. He has had no shortness of breath, palpitations, fevers, or chills. He emigrated from Ecuador when he was 5 years old. He does not smoke or drink alcohol. He takes no medications. He is 194 cm (6 ft 4 in) tall and weighs 70.3 kg (155 lb); BMI is 19 kg/m2. His temperature is 37.2°C (99.0°F), pulse is 73/min, respirations are 15/min, and blood pressure is 152/86 mm Hg in the right arm and 130/72 mm Hg in the left arm. Pulmonary examination shows faint inspiratory wheezing bilaterally. A CT scan of the chest with contrast is shown. Which of the following is the most likely underlying cause of this patient's condition?
A 58-year-old man presents to the emergency department with severe chest pain and uneasiness. He says that symptoms onset acutely half an hour ago while he was watching television. He describes the pain as being 8/10 in intensity, sharp in character, localized to the center of the chest and retrosternal, and radiating to the back and shoulders. The patient denies any associated change in the pain with breathing or body position. He says he has associated nausea but denies any vomiting. He denies any recent history of fever, chills, or chronic cough. His past medical history is significant for hypertension, hyperlipidemia, and diabetes mellitus for which he takes lisinopril, hydrochlorothiazide, simvastatin, and metformin. He reports a 30-pack-year smoking history and has 1–2 alcoholic drinks during the weekend. Family history is significant for hypertension, hyperlipidemia, and an ST elevation myocardial infarction in his father and paternal uncle. His blood pressure is 220/110 mm Hg in the right arm and 180/100 mm Hg in the left arm. On physical examination, the patient is diaphoretic. Cardiac exam reveals a grade 2/6 diastolic decrescendo murmur loudest over the left sternal border. Remainder of the physical examination is normal. The chest radiograph shows a widened mediastinum. The electrocardiogram (ECG) reveals non-specific ST segment and T wave changes. Intravenous morphine and beta-blockers are started. Which of the following is the most likely diagnosis in this patient?
A 55-year-old man presents to the emergency department for chest pain. He states that the pain started last night and has persisted until this morning. He describes the pain as in his chest and radiating into his back between his scapulae. The patient has a past medical history of alcohol abuse and cocaine abuse. He recently returned from vacation on a transatlantic flight. The patient has smoked 1 pack of cigarettes per day for the past 20 years. His temperature is 99.5°F (37.5°C), blood pressure is 167/118 mmHg, pulse is 120/min, and respirations are 22/min. Physical exam reveals tachycardia and clear air movement bilaterally on cardiopulmonary exam. Which of the following is also likely to be found in this patient?
A 71-year old man is brought to the emergency department because of progressively worsening shortness of breath and fatigue for 3 days. During the last month, he has also noticed dark colored urine. He had an upper respiratory infection 6 weeks ago. He underwent a cholecystectomy at the age of 30 years. He has hypertension, hyperlipidemia, and type 2 diabetes mellitus. He immigrated to the US from Italy 50 years ago. Current medications include simvastatin, lisinopril, and metformin. He appears pale. His temperature is 37.1°C (98.8°F), pulse is 96/min, respirations are 21/min, and blood pressure is 150/80 mm Hg. Auscultation of the heart shows a grade 4/6 systolic murmur over the right second intercostal space that radiates to the carotids. Laboratory studies show: Leukocyte count 9,000/mm3 Hemoglobin 8.3 g/dL Hematocrit 24% Platelet count 180,000/mm3 LDH 212 U/L Haptoglobin 15 mg/dL (N=41–165) Serum Na+ 138 mEq/L K+ 4.5 mEq/L CL- 102 mEq/L HCO3- 24 mEq/L Urea nitrogen 20 mg/dL Creatinine 1.2 mg/dL Total bilirubin 1.8 mg/dL Stool testing for occult blood is negative. Direct Coombs test is negative. Echocardiography shows an aortic jet velocity of 4.2 m/s and a mean pressure gradient of 46 mm Hg. Which of the following is the most appropriate next step in management to treat this patient's anemia?
A 69-year-old man is brought to the emergency room by his wife 30 minutes after losing consciousness while they were working in their garden together. The patient says that time seemed to slow down, his vision went dark, and he had a sensation of falling. After 3–5 seconds, he awoke slightly disoriented but quickly regained his baseline mental status. The patient says he has had a few similar episodes that occurred 1–2 months ago for which he did not seek any medical treatment. He says overall he has been more tired than usual and feeling out of breath on his morning walks. He denies any chest pain or palpitations. Past medical history is significant for type 1 diabetes mellitus. Current medications are atorvastatin and insulin. His family history is significant for his father who died of myocardial infarction in his 70’s. His blood pressure is 110/85 mm Hg and pulse is 82/min. On physical examination, there is a 3/6 systolic murmur best heard over the right sternal border with radiation to the carotids. S1 is normal but there is a soft unsplit S2. The lungs are clear to auscultation bilaterally. The remainder of the exam is unremarkable. Which of the following physical exam findings would also most likely be present in this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app