
Arrhythmias — MCQs

On this page
A 24-year-old woman presents to the emergency department with palpitations for the last hour. This is her 3rd emergency department visit in the last 8 weeks due to the same complaint. She denies fever, shortness of breath, nasal discharge, bowel changes, weight loss, and heat intolerance. She has asthma that is poorly controlled despite regular inhaler use. She drinks a cup of coffee each morning, and she is physically active and jogs for at least 30 minutes daily. She is in a monogamous relationship with her boyfriend and regularly uses barrier contraceptives. Her last menses was 1 week ago. Physical examination reveals: blood pressure 104/70 mm Hg, pulse 194 /min that is regular, and respiratory rate 18/min. Her ECG is shown in the image. A gentle massage over the carotid artery for 5–10 seconds did not terminate her palpitations. What is the most appropriate next step in the management of this patient?
A 43-year-old woman presents to a physician with weakness and fatigue for a week. She mentions that she has been taking oral fluconazole for the last 4 weeks for the treatment of tinea capitis. She also says that she loves coffee and usually consumes 4–6 cups of coffee every day. On physical examination, her vital signs are stable and examination of all systems, including nervous system, is normal. Her laboratory evaluation reveals that her serum potassium level is 3.1 mmol/L (3.1 mEq/L). The physician orders an ECG. Which of the following findings is most likely to be present?
A 27-year-old man presents to the emergency department with a progressively worsening cough, wheezes, and chest tightness over the last 2 days. He has a history of moderate persistent asthma and his maintenance regimen consists of an inhaled corticosteroid, a long-acting beta-agonist, and albuterol as rescue therapy. He has not improved with his rescue inhaler despite increased use. He reports prior exposure to a person who had symptoms of a respiratory infection. His temperature is 37.4°C (99.3°F), blood pressure is 101/68 mm Hg, heart rate is 99/min, and respiratory rate is 32/min. Physical examination reveals widespread polyphonic wheezes but equal air entry. His oxygen saturation is 92% on room air. The presence of which of the following categorizes this patient’s condition as life-threatening?
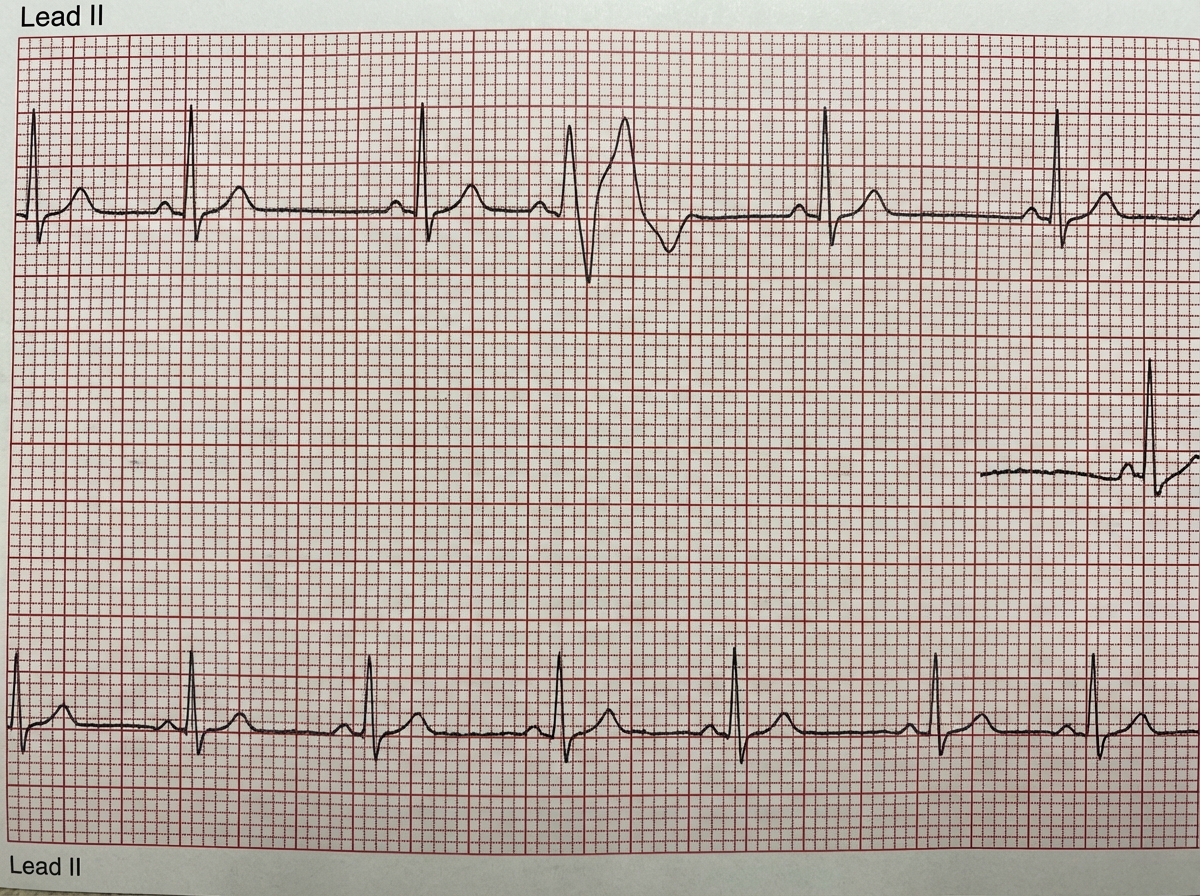
A 26-year-old man comes to the physician because of episodic palpitations for the past 2 months. He has the feeling that sometimes his heart “skips a beat”. His father has a history of atrial fibrillation and myocardial infarction. He has smoked one pack of cigarettes daily for 5 years. He drinks 1–2 beers on the weekends. His vital signs are within normal limits. Physical examination reveals a regular pulse. Cardiopulmonary examination shows no abnormalities. Serum studies, including electrolytes and creatinine, are within normal limits. An excerpt of 24h Holter monitoring is shown. Echocardiography is normal. Which of the following is the most appropriate next step in management?
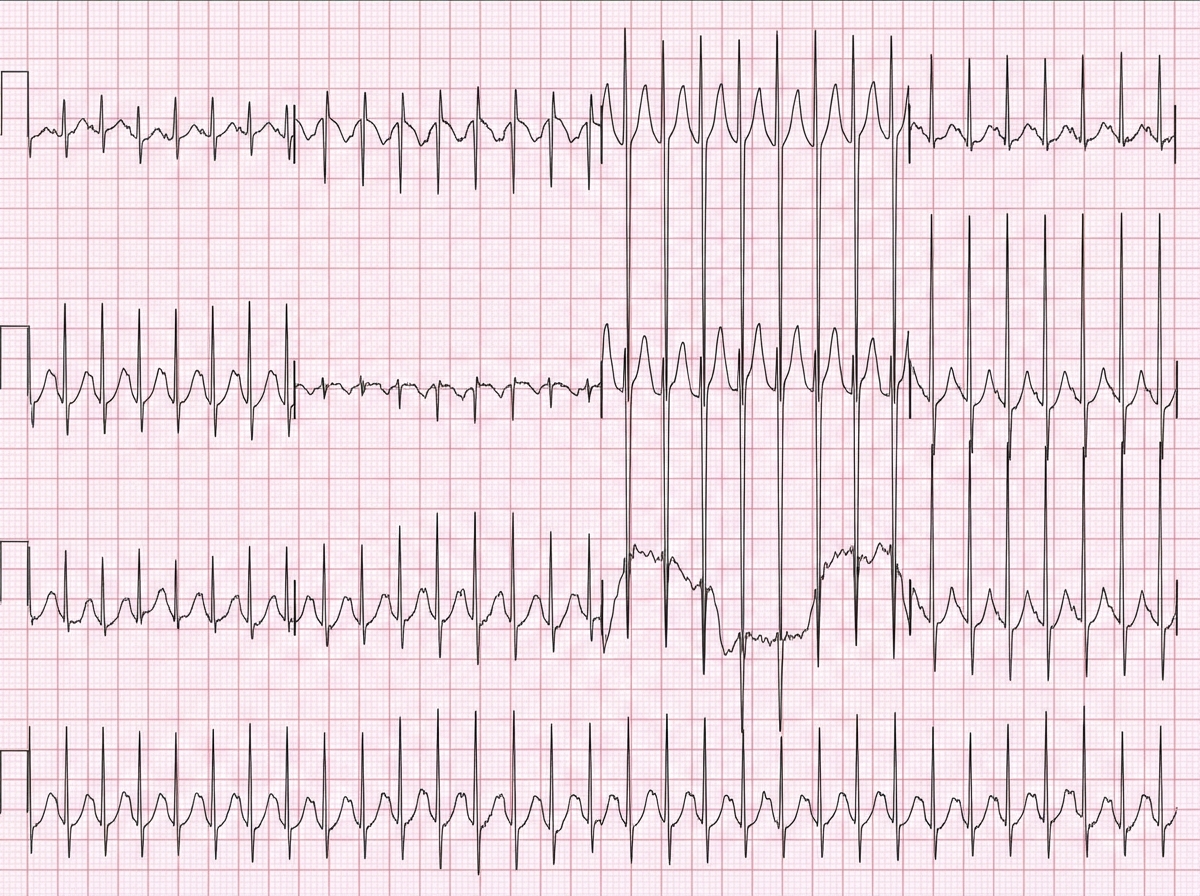
A 23-year-old man comes to the emergency department because of palpitations, dizziness, and substernal chest pain for three hours. The day prior, he was at a friend’s wedding, where he consumed seven glasses of wine. The patient appears diaphoretic. His pulse is 220/min and blood pressure is 120/84 mm Hg. Based on the patient's findings on electrocardiography, the physician diagnoses atrial fibrillation with rapid ventricular response and administers verapamil for rate control. Ten minutes later, the patient is unresponsive and loses consciousness. Despite resuscitative efforts, the patient dies. Histopathologic examination of the heart at autopsy shows an accessory atrioventricular conduction pathway. Electrocardiography prior to the onset of this patient's symptoms would most likely have shown which of the following findings?
A 55-year-old man with a past medical history of obesity and hyperlipidemia suddenly develops left-sided chest pain and shortness of breath while at work. He relays to coworkers that the pain is intense and has spread to his upper left arm over the past 10 minutes. He reports it feels a lot like the “heart attack” he had a year ago. He suddenly collapses and is unresponsive. Coworkers perform cardiopulmonary resuscitation for 18 minutes until emergency medical services arrives. Paramedics pronounce him dead at the scene. Which of the following is the most likely cause of death in this man?
A 62-year-old man is brought to the emergency department because of syncope. He reports sudden onset of palpitations followed by loss of consciousness while carrying his groceries to his car. He is unable to recall any further details and does not have any chest pain or dizziness. He has a history of hypertension, type 2 diabetes mellitus, gastroparesis, and osteoarthritis of the knees. Medications include lisinopril, metformin, and ondansetron as needed for nausea. He also takes methadone daily for chronic pain. Apart from an abrasion on his forehead, he appears well. His temperature is 37.2 °C (98.9 F), heart rate is 104/min and regular, and blood pressure is 135/70 mm Hg. While he is in the emergency department, he loses consciousness again. Telemetry shows polymorphic ventricular tachycardia with cyclic alteration of the QRS axis that spontaneously resolves after 30 seconds. Results of a complete blood count, serum electrolyte concentrations, and serum thyroid studies show no abnormalities. Cardiac enzymes are within normal limits. Which of the following is the most likely underlying cause of this patient's syncope?
A 45-year-old woman comes to the physician because of multiple episodes of dizziness over the past 3 months. Episodes last between 20 minutes and 1 hour. During the episodes she experiences the sudden onset of spinning sensations and imbalance, associated with a ringing in her left ear. She also reports progressive left-sided hearing loss and is unable to follow conversations in noisy surroundings. She has had an upper respiratory infection for the past 5 days, which is being treated with erythromycin. She has been otherwise healthy. Her vital signs are within normal limits. Examination shows no abnormalities. Pure tone audiometry shows a combined low- and high-frequency sensory loss of the left ear with normal hearing in the mid frequencies. Which of the following is the most appropriate initial step in management?
Practice by Chapter
Basic electrophysiology
Practice Questions
ECG interpretation fundamentals
Practice Questions
Supraventricular tachycardias
Practice Questions
Atrial fibrillation and flutter
Practice Questions
Ventricular arrhythmias
Practice Questions
Bradyarrhythmias and conduction disorders
Practice Questions
Sudden cardiac death
Practice Questions
Antiarrhythmic medications
Practice Questions
Cardioversion and defibrillation
Practice Questions
Pacemakers and ICDs
Practice Questions
Catheter ablation procedures
Practice Questions
Secondary arrhythmias (electrolyte, drug-induced)
Practice Questions
Inherited arrhythmia syndromes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app