
Arrhythmias — MCQs

On this page
A 71-year-old female is brought to the emergency room by her husband. The husband reports that they were taking a walk together one hour ago, when his wife experienced sudden, right arm and leg weakness. He noticed that she had slurred speech, and that she was not able to tell him where she was. The patient underwent an emergent CT scan, which was unremarkable, and was treated with tissue plasminogen activator (tPA). Which of the following EKG findings increases a patient's risk for this acute presentation?
A 57-year-old man comes to the emergency department with fatigue and palpitations for several weeks. An ECG shows atrial fibrillation. Echocardiography shows thrombus formation in the left atrium. Which of the following organs is most likely to continue to function in the case of an embolic event?
A 22-year-old medical student presents to a community health center due to an episode of loss of consciousness 3 days ago. She also has a history of multiple episodes of dizziness in the last year. These episodes almost always occur when she is observing surgery in the operating room. She describes her dizziness as a feeling of lightheadedness, warmth, excessive sweating, and palpitations. She feels that she will fall down if she stood longer and usually sits on the floor or leaves the room until the feeling subsides. Three days ago, she collapsed while observing an open cholecystectomy but regained consciousness after a few seconds. Once she regained consciousness, she was pale and sweating excessively. Her medical history is significant for migraines, but she is not on prophylactic therapy. Her younger brother has cerebral palsy, and her uncle had a sudden death at the age of 25. Her blood pressure is 120/80 mm Hg when lying down and 118/80 mm Hg when in a standing position. The rest of the physical examination is within normal limits. What is the next best step in the management of this patient?
A 31-year-old woman with a history of anorexia nervosa diagnosed 2 years ago presents for follow up. She says that, although she feels some improvement with cognitive-behavioral therapy (CBT), she is still struggling with her body image and fears gaining weight. She says that for the past 3 weeks she has noticed her ankles are uncomfortably swollen in the mornings. She also mentions that she still is having intermittent menstruation; her last menstrual cycle was 4 months ago. The patient denies any suicidal ideations. She has no other significant past medical history. She denies any history of smoking, alcohol consumption, or recreational drug use. The patient’s vital signs include: temperature 37.0°C (98.6°F), pulse 55/min, blood pressure 100/69 mm Hg, and respiratory rate 18/min. Her body mass index (BMI) is 17.1 kg/m2, improved from 16.9 kg/m2, 6 months ago. Her physical examination is significant for an irregular heart rhythm on cardiopulmonary auscultation. There is also significant 3+ pitting edema in the lower extremities bilaterally. An ECG reveals multiple isolated premature ventricular contractions (PVCs) with 1 10-sec episode of bigeminy. Which of the following aspects of this patient’s history and physical examination would be the strongest indication for inpatient hospitalization?
A 58-year-old man complains of ascending weakness, palpitations, and abdominal pain. He has a history of hypertension, type II diabetes mellitus, diabetic retinopathy, and end-stage renal disease requiring dialysis. He denies any recent infection. Physical examination is notable for decreased motor strength in both his upper and lower extremities, intact cranial nerves, as well as decreased bowel sounds. On further questioning, the patient shares that he has been depressed, as he feels he may not be able to see his grandchildren grow due to his complicated medical course. This caused him to miss two of his dialysis appointments. Which of the following will mostly likely be found on electrocardiography?
A 33-year-old African American woman presents to her primary care physician for a wellness checkup. She states that she has lost 20 pounds over the past 2 months yet has experienced an increased appetite during this period. She endorses hyperhidrosis and increased urinary volume and frequency. Physical exam is notable for an anxious woman and a regular and tachycardic pulse. Laboratory values are ordered as seen below. Serum: Na+: 139 mEq/L Cl-: 100 mEq/L K+: 4.3 mEq/L HCO3-: 25 mEq/L Ca2+: 12.2 mg/dL The patient's urine calcium level is elevated. Which of the following is the most likely diagnosis?
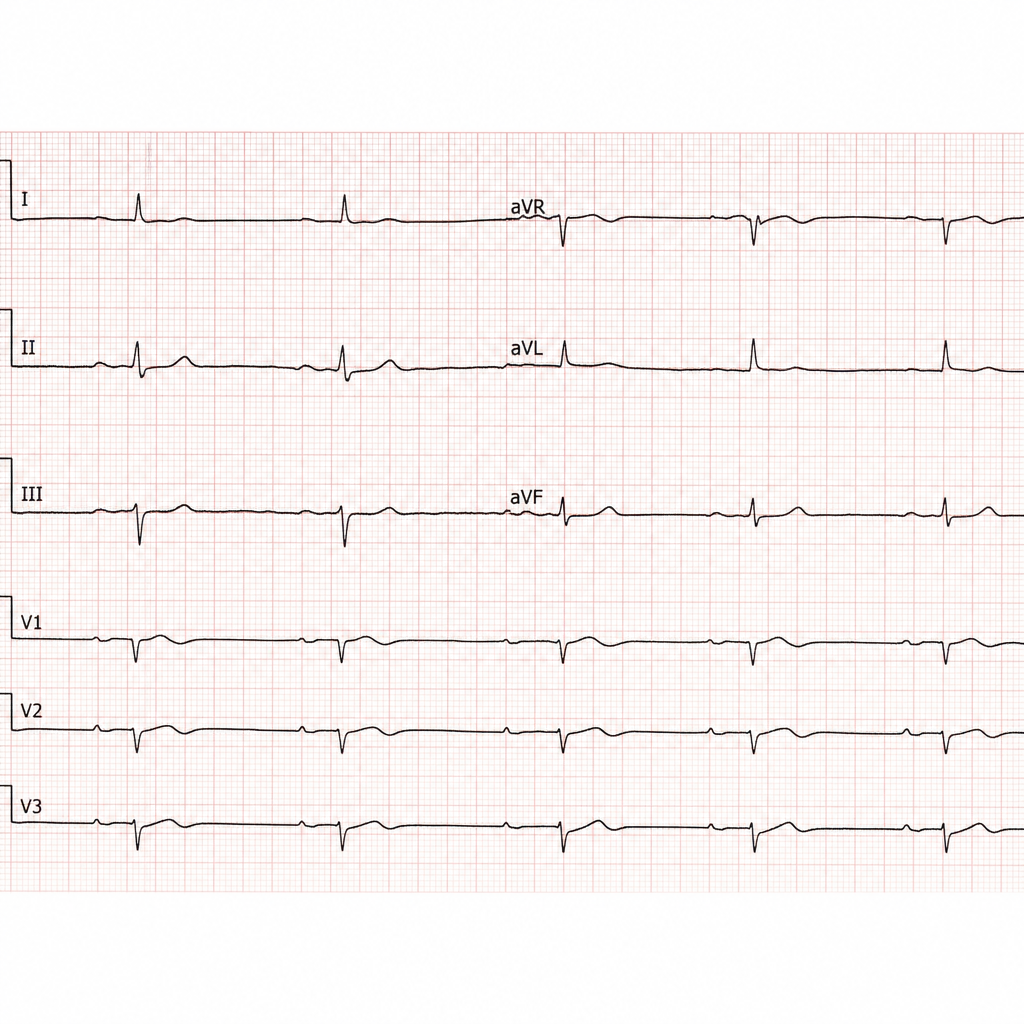
A 69-year-old man presents to his primary care physician after 2 episodes of dizziness while watching television. On further questioning, he admits to progressive fatigue and shortness of breath on exertion for the past few weeks. His medical history is significant for hypertension for the past 25 years and congestive heart failure for the past 2 years, for which he is on multiple medications. His blood pressure is 100/50 mm Hg, the heart rate is 50/min, and the temperature is 36.6°C (97.8°F). The physical examination is within normal limits. A 12-lead ECG is obtained and the results are shown in the picture. Which of the following is the best initial step for the management of this patient?
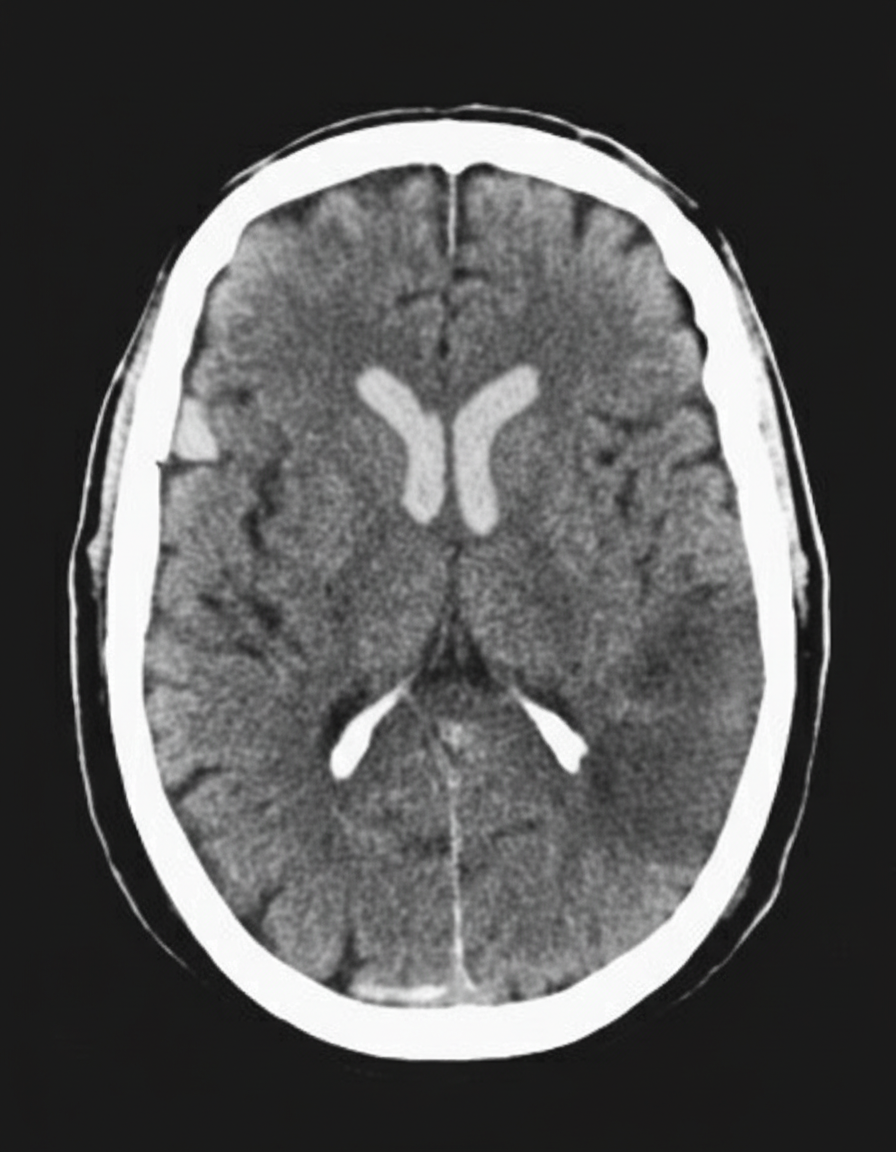
A 45-year-old man presents to the emergency department with complaints of right-sided weakness and slurring of speech for 1 hour. There is no history of head trauma, myocardial infarction, recent surgery, gastrointestinal or urinary bleeding. He has hypertension, chronic atrial fibrillation, and a 20 pack-year cigarette smoking history. The medication list includes valsartan and rivaroxaban, which he took within the previous 48 hours and has clinically significant anticoagulant activity on a rivaroxaban-calibrated anti-factor Xa assay. The vital signs include: blood pressure 180/92 mm Hg, pulse 144/min and irregular, and temperature 37.2°C (99.0°F). On physical examination, there is a facial asymmetry with a deviation of angle of mouth to the left side on smiling. Muscle strength is reduced in both upper and lower limbs on the right side while on the left side it's normal. Random blood glucose is 104 mg/dL. A complete blood count is normal. A CT scan of the head is shown in the image. What is the most appropriate next step in the management of this patient?
A 65-year-old woman is brought to the emergency department by her husband due to difficulty speaking and confusion for 1 hour. She was gardening when she suddenly developed these symptoms. She is not able to respond to the questions despite multiple repetitions. She also appears unsteady with her gait and is able to walk with support. The past medical history includes type 2 diabetes mellitus, dyslipidemia, and osteoarthritis. The medicine list includes aspirin, atorvastatin, metformin, and chondroitin sulfate. The vital signs include: blood pressure 174/88 mm Hg, heart rate 154/min and irregular, respiratory rate 12/min, and oxygen saturation 96% on room air. She is awake, but not following commands. The pupils are equal bilaterally and reactive to light. There is mild facial droop on the right side. The forehead wrinkles are preserved. When the soles of her feet are stimulated with a blunt instrument, the right-sided big toe goes upward, while the left-sided big toe goes downward. The ECG shows variable R-R intervals and absence of P waves. What is the next step in the management of this patient?
A 75-year-old man presents to the emergency department after an episode of syncope while walking outside with his wife. His wife states that he suddenly appeared pale and collapsed to the ground. She says he remained unconscious for 1 minute. He says he noticed a fluttering in his chest and excessive sweating before the episode. He has type 2 diabetes mellitus, essential hypertension, and chronic stable angina. He has not started any new medications in the past few months. Vital signs reveal: temperature 37.0°C (98.6°F), blood pressure 135/72 mm Hg, and pulse 72/min. Physical examination is unremarkable. ECG shows an old bifascicular block. Echocardiogram and 24-hour Holter monitoring are normal. Which of the following is the best next step in the evaluation of this patient's condition?
Practice by Chapter
Basic electrophysiology
Practice Questions
ECG interpretation fundamentals
Practice Questions
Supraventricular tachycardias
Practice Questions
Atrial fibrillation and flutter
Practice Questions
Ventricular arrhythmias
Practice Questions
Bradyarrhythmias and conduction disorders
Practice Questions
Sudden cardiac death
Practice Questions
Antiarrhythmic medications
Practice Questions
Cardioversion and defibrillation
Practice Questions
Pacemakers and ICDs
Practice Questions
Catheter ablation procedures
Practice Questions
Secondary arrhythmias (electrolyte, drug-induced)
Practice Questions
Inherited arrhythmia syndromes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app