
Arrhythmias — MCQs

On this page
A 32-year-old woman presents to the emergency department with unilateral vision loss. She states it started suddenly this evening and this has never happened to her before. The patient is not followed by a primary care physician and is not currently taking any medications. She has had a few episodes of weakness or numbness in the past but states her symptoms usually resolve on their own. Her temperature is 97.6°F (36.4°C), blood pressure is 120/74 mmHg, pulse is 88/min, respirations are 12/min, and oxygen saturation is 98% on room air. Physical exam is notable for decreased sensation over the patient's dorsal aspect of her left foot. Visual exam reveals a loss of vision in the patient's left eye and she endorses pain in the eye on exam. Which of the following findings is also likely to be found in this patient?
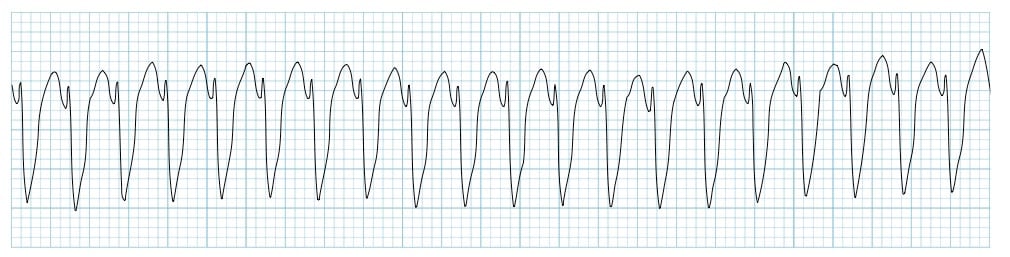
Two days after admission for myocardial infarction and subsequent coronary angioplasty, a 65-year-old man becomes distressed and diaphoretic in the cardiac intensive care unit. Suddenly he is no longer responsive. Pulse oximetry does not show a tracing. He has a history of hypertension and depression. Prior to his admission, his medication included ramipril and aripiprazole. Examination shows no carotid pulse. An ECG is shown. After beginning chest compressions, which of the following is the most appropriate step in management of the patient?
A 15-year-old boy is brought to the emergency department after he passed out in the hallway. On presentation, he is alert but confused about why he is in the hospital. He says that he remembers seeing flashes of light to his right while walking out of class but cannot recall what happened next. His next memory is being woken up by emergency responders who wheeled him into an ambulance. A friend who was with him at the time says that he seemed to be swallowing repeatedly and staring out into space. He has never had an episode like this before, and his past medical history is unremarkable. Which of the following characteristics is most likely true of the cause of this patient's symptoms?
A 28-year-old man presents to the emergency department with lower extremity weakness. He was in his usual state of health until 10 days ago. He then began to notice his legs were “tiring out” during his workouts. This progressed to difficulty climbing the stairs to his apartment. He has asthma and uses albuterol as needed. He has no significant surgical or family history. He smokes marijuana daily but denies use of other recreational drugs. He is sexually active with his boyfriend of 2 years. He has never traveled outside of the country but was camping 3 weeks ago. He reports that he had diarrhea for several days after drinking unfiltered water from a nearby stream. On physical examination, he has 1/5 strength in his bilateral lower extremities. He uses his arms to get up from the chair. Achilles and patellar reflexes are absent. A lumbar puncture is performed, and results are as shown below: Cerebral spinal fluid: Color: Clear Pressure: 15 cm H2O Red blood cell count: 0 cells/µL Leukocyte count: 3 cells/ µL with lymphocytic predominance Glucose: 60 mg/dL Protein: 75 mg/dL A culture of the cerebral spinal fluid is pending. Which of the following is the part of the management for the patient’s most likely diagnosis?
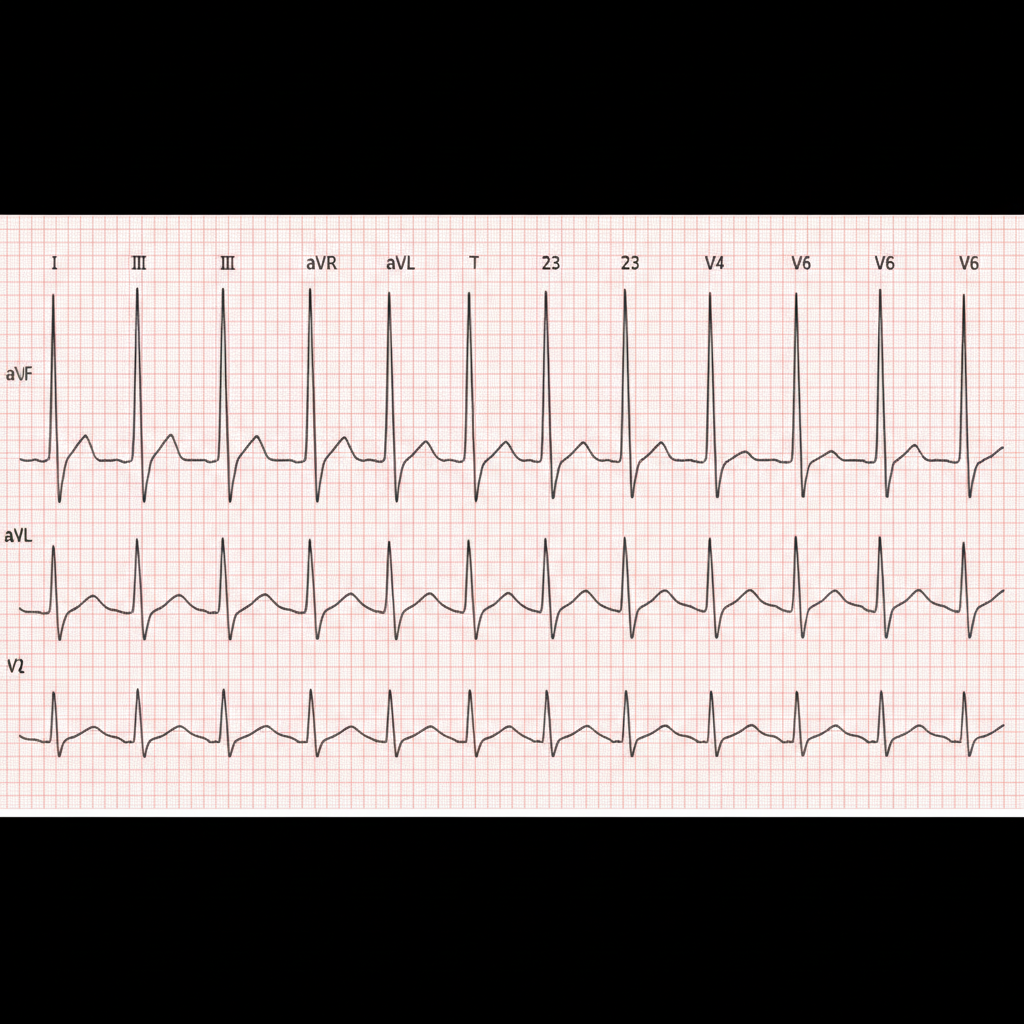
A 77-year-old man presents to his primary care physician with lightheadedness and a feeling that he is going to "pass out". He has a history of hypertension that is treated with captopril. In the office, his temperature is 38.3°C (100.9°F), the pulse is 65/min, and the respiratory rate is 19/min. His sitting blood pressure is 133/91 mm Hg. Additionally, his supine blood pressure is 134/92 mm Hg and standing blood pressure is 127/88 mm Hg. These are similar to his baseline blood pressure measured during previous visits. An ECG rhythm strip is obtained in the office. Of the following, what is the likely cause of his presyncope?
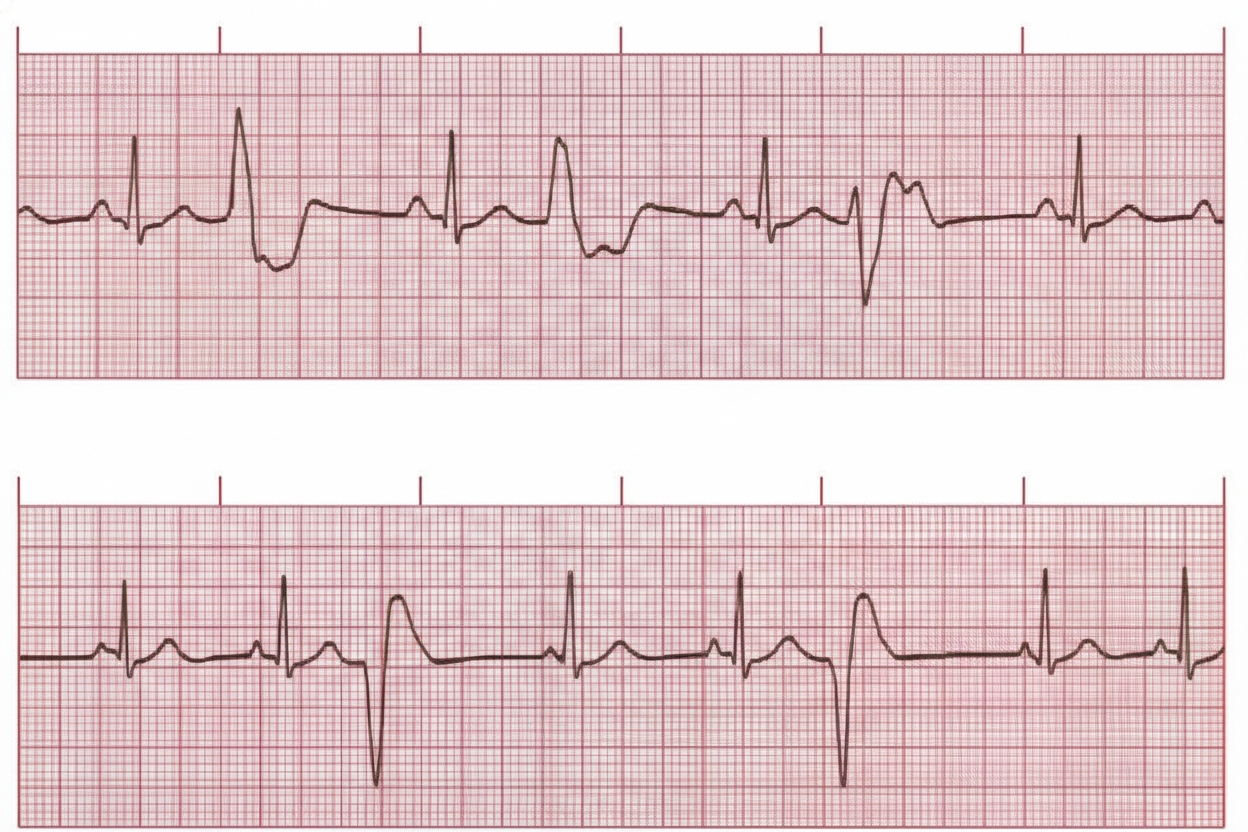
A 24-year-old woman comes to the physician for a routine health maintenance examination. She feels well. On questioning, she has had occasional mild morning dizziness (not presyncope) and non-bothersome palpitations during the past year. She is a graduate student. She does not smoke and drinks 1–2 glasses of wine on the weekends. There is no family history of sudden cardiac death. Her vital signs are within normal limits. Physical examination shows an irregular pulse with no signs of structural heart disease; S1 and S2 are normal and there are no murmurs. An ECG is shown demonstrating infrequent unifocal premature ventricular contractions. Which of the following is the most appropriate next step in management?
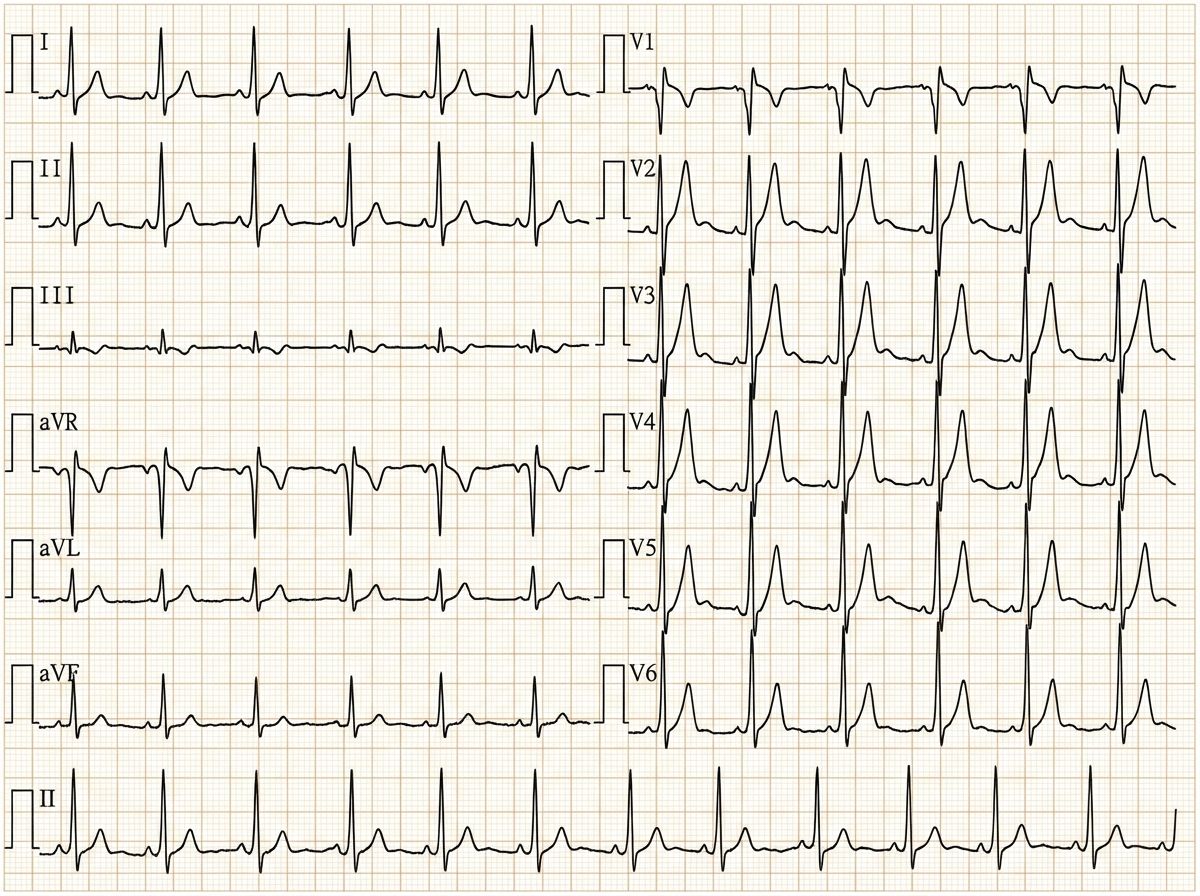
A 62-year-old woman presents to the emergency department complaining of fever, worsening fatigue, and muscle weakness for the previous 48 hours. The patient describes her muscle weakness as symmetric and worse in the upper limbs. Her past medical history is significant for long-standing diabetes type 2 complicated by stage 5 chronic kidney disease (CKD) on hemodialysis. She takes lisinopril, verapamil, and glargine. Today, the patient's vital signs include: temperature 38.6°C (101.5°F), pulse 80/min, blood pressure 155/89 mm Hg, respirations 24/min, and 95% oxygen saturation on room air. The cardiac and pulmonary exams are unremarkable. The abdomen is soft and non-tender. Her strength is 3/5 in the upper extremities and 4/5 in the lower extremities and her sensation is intact. Deep tendon reflexes are absent in both the upper and lower limbs. A 12-lead electrocardiogram (ECG) is shown in the image below, demonstrating diffuse narrow peaked T waves consistent with hyperkalemic cardiotoxicity. Blood work is drawn and the patient is admitted and started on continuous cardiac monitoring. Based on the available information, what is the next best step in managing this patient?
A 64-year-old male presents to the emergency room complaining of chest pain. He reports a pressure-like sensation over his sternum that radiates into his jaw. The pain came on suddenly 2 hours ago and has been constant since then. His past medical history is notable for a stable abdominal aortic aneurysm, hypertension, diabetes, and hyperlipidemia. He takes aspirin, enalapril, spironolactone, atorvastatin, canagliflozin, and metformin. His temperature is 99.1°F (37.3°C), blood pressure is 155/85 mmHg, pulse is 115/min, and respirations are 22/min. On exam, he is diaphoretic and in moderate distress. He is admitted for further management and does well after initial stabilization. He is seen two days later by the admitting team. This patient is at increased risk for a complication that is characterized by which of the following?
A 26-year-old nursing home staff presents to the emergency room with complaints of palpitations and chest pain for the past 2 days. She was working at the nursing home for the last year but has been trying to get into modeling for the last 6 months and trying hard to lose weight. She is a non-smoker and occasionally drinks alcohol on weekends with friends. On examination, she appears well nourished and is in no distress. The blood pressure is 150/84 mm Hg and the pulse is 118/min. An ECG shows absent P waves. All other physical findings are normal. What is the probable diagnosis?
A 29-year-old woman with Wolff-Parkinson-White syndrome presents to her cardiologist’s office for a follow-up visit. She collapsed at her job and made a trip to the emergency department 1 week ago. At that time, she received a diagnosis of atrial fibrillation with rapid ventricular response and hemodynamic instability. While in the emergency department, she underwent direct-current cardioversion to return her heart to sinus rhythm. Her current medications include procainamide. At the cardiologist’s office, her heart rate is 61/min, respiratory rate is 16/min, the temperature is 36.5°C (97.7°F), and blood pressure is 118/60 mm Hg. Her cardiac examination reveals a regular rhythm and a I/VI systolic ejection murmur best heard at the right upper sternal border. An ECG obtained in the clinic is shown. Which of the following is the most appropriate treatment to prevent further episodes of tachyarrhythmia?
Practice by Chapter
Basic electrophysiology
Practice Questions
ECG interpretation fundamentals
Practice Questions
Supraventricular tachycardias
Practice Questions
Atrial fibrillation and flutter
Practice Questions
Ventricular arrhythmias
Practice Questions
Bradyarrhythmias and conduction disorders
Practice Questions
Sudden cardiac death
Practice Questions
Antiarrhythmic medications
Practice Questions
Cardioversion and defibrillation
Practice Questions
Pacemakers and ICDs
Practice Questions
Catheter ablation procedures
Practice Questions
Secondary arrhythmias (electrolyte, drug-induced)
Practice Questions
Inherited arrhythmia syndromes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app