
Arrhythmias — MCQs

On this page
A 32-year-old man is brought to the emergency department after a car accident; he was extricated after 4 hours. He did not lose consciousness and does not have headache or nausea. He is in severe pain. He sustained severe injuries to both arms and the trauma team determines that surgical intervention is needed. Urinary catheterization shows dark colored urine. His temperature is 38°C (100.4°F), pulse is 110/min, and blood pressure is 90/60 mm Hg. The patient is alert and oriented. Examination shows multiple injuries to the upper extremities, contusions on the trunk, and abdominal tenderness. Laboratory studies show: Hemoglobin 9.2 g/dL Leukocyte count 10,900/mm3 Platelet count 310,000/mm3 Serum Na+ 137 mEq/L K+ 6.8 mEq/L Cl- 97 mEq/L Glucose 168 mg/dL Creatinine 1.7 mg/dL Calcium 7.7 mg/dL Arterial blood gas analysis on room air shows a pH of 7.30 and a serum bicarbonate of 14 mEq/L. An ECG shows peaked T waves. A FAST scan of the abdomen is negative. Two large bore cannulas are inserted and intravenous fluids are administered. Which of the following is the most appropriate next step in management?
A 31-year-old nurse presents to the emergency department with palpitations, sweating, and jitteriness. She denies chest pain, shortness of breath, and recent illness. She states that she experienced weakness in her arms and legs and a tingling sensation in her fingers before the palpitations occurred. Medical and surgical history is unremarkable. Her mother has Grave’s disease. The patient has been seen in the ED multiple times for similar symptoms and was discharged after appropriate medical management. Today, her temperature is 37°C (98.6°F), blood pressure is 128/84 mm Hg, pulse is 102/min and regular, and respirations are 10/min. On examination, the patient appears diaphoretic and anxious. Her pupils are dilated to 5 mm. The rest of the examination is normal. Urine toxicology and B-HCG are pending. Which of the following is the next best step in management?
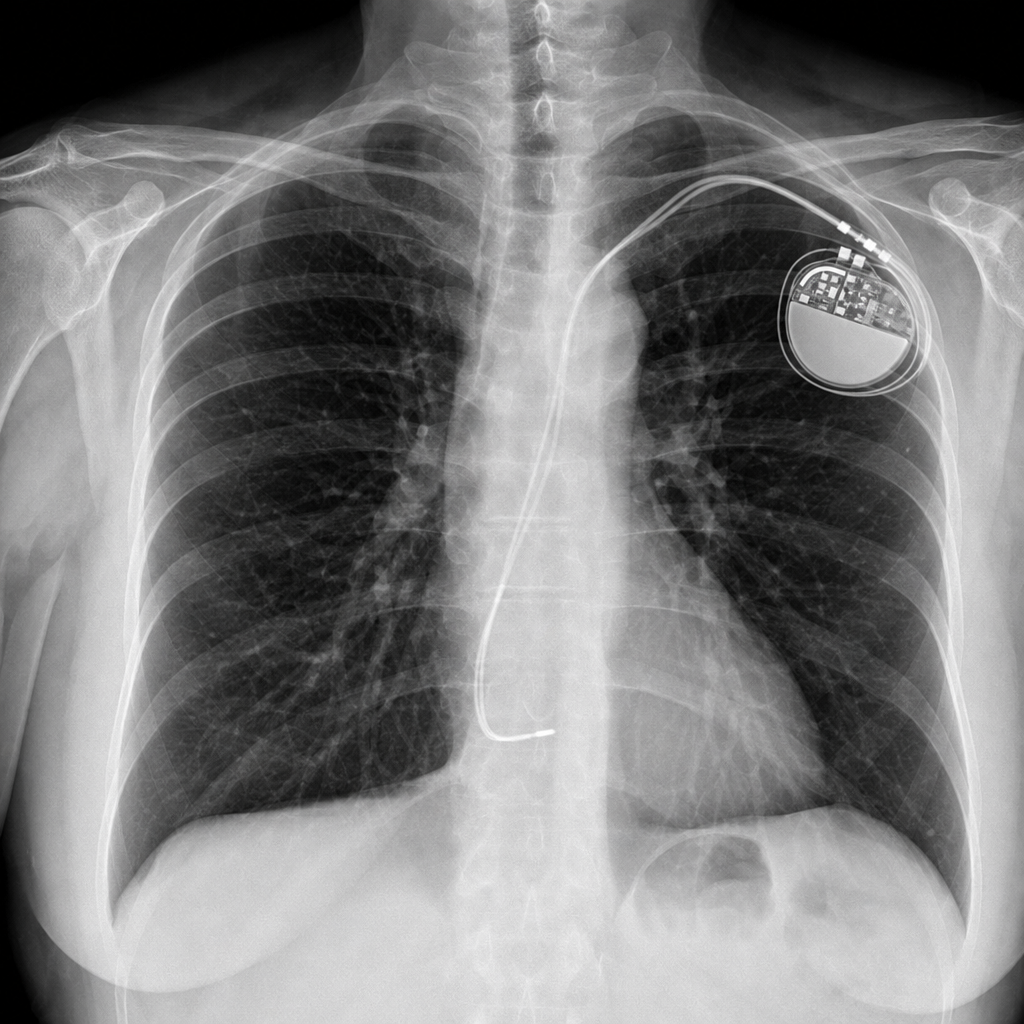
A 67-year-old woman comes to the emergency department because of a 4-month history of fatigue, shortness of breath with exertion, and dizziness. She has a history of atrial fibrillation and had a single-chamber pacemaker placed five years ago after an episode of syncope. Her pulse is 66/min and blood pressure is 98/66 mm Hg. An x-ray of the chest is shown. The x-ray confirms termination of the pacemaker lead in which of the following structures?
A 25-year-old man presents to the emergency department complaining of palpitations, lightheadedness, and sweating. He just started working at an investment firm and has been working long hours to make a good impression. Today, he had a dozen cups of espresso to keep himself awake and working. He has never had such an episode before. His past medical history is unremarkable. His pulse is 150/min, blood pressure is 134/88 mm Hg, respirations are 12/min, and temperature is 36.7°C (98.0°F). ECG shows supraventricular tachycardia. Which of the following is the next best step in the management of this patient?
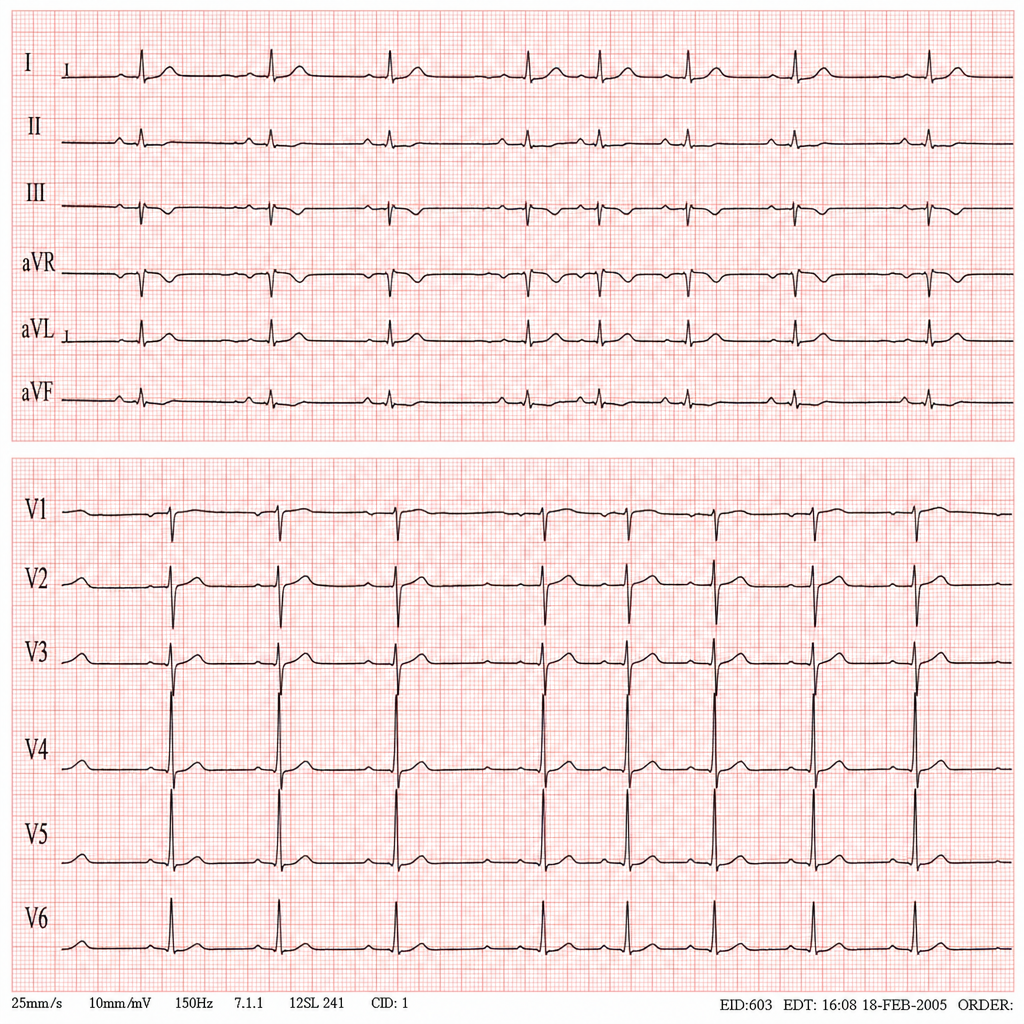
A 45-year-old man comes to the physician for a routine health maintenance examination. He feels well. He underwent appendectomy at the age of 25 years. He has a history of hypercholesterolemia that is well controlled with atorvastatin. He is an avid marathon runner and runs 8 miles per day four times a week. His father died of myocardial infarction at the age of 42 years. The patient does not smoke or drink alcohol. His vital signs are within normal limits. Cardiopulmonary examination shows no abnormalities. His abdomen is soft and nontender with a surgical scar in the right lower quadrant. Laboratory studies are within normal limits. An ECG is shown. Which of the following is the most likely diagnosis?
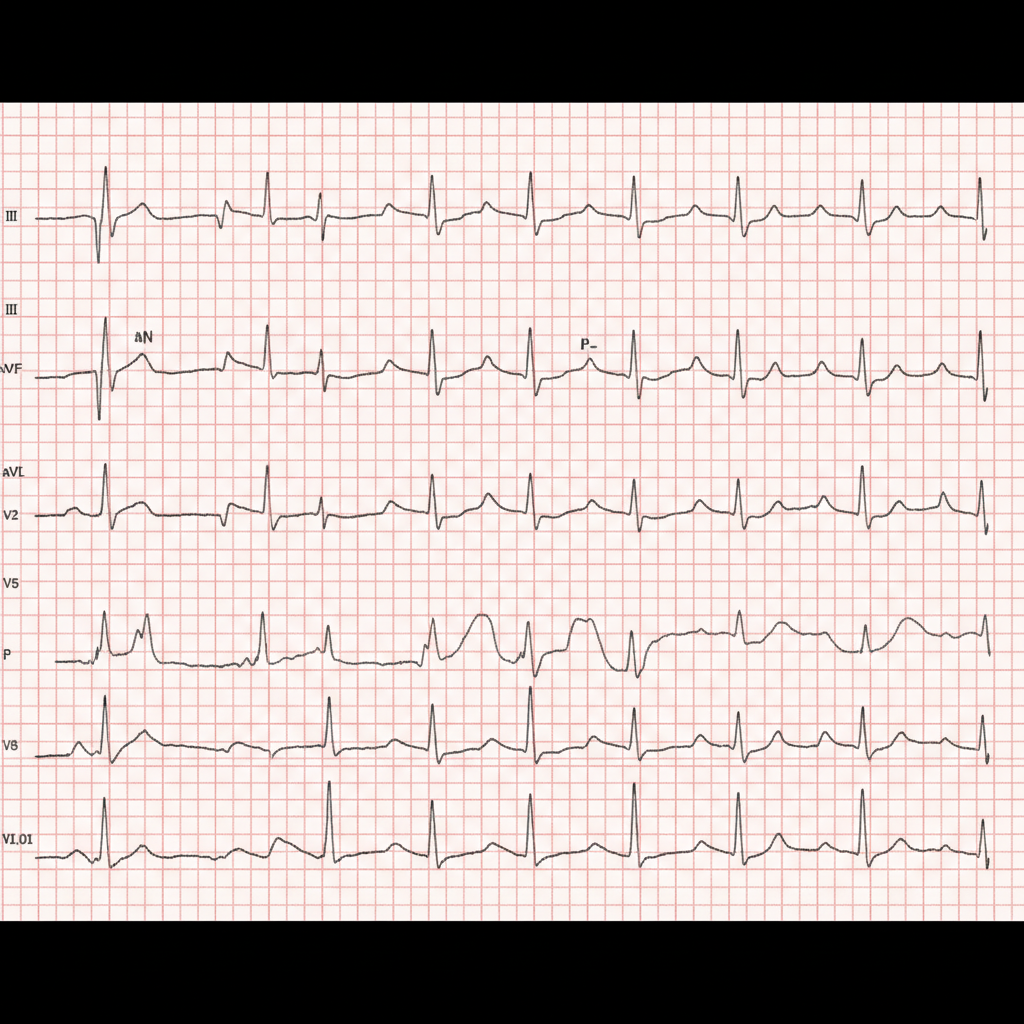
A 68-year-old man presents to the emergency department because of difficulty breathing and chest tightness for the last 3 days. He also has a productive cough with excessive amounts of green sputum. He has had chronic obstructive pulmonary disease for the past 10 years, but says that the cough and sputum are different compared to his baseline. He took 2 doses of nebulized albuterol and ipratropium at home, but that did not completely relieve his symptoms. He has a 50 pack-year smoking history and drinks alcohol occasionally. His vital signs include a blood pressure of 110/60 mm Hg, a temperature of 37.2 °C (98.9°F), a respiratory rate of 26/min, an irregular radial pulse at a rate of 110–120/min, and an oxygen saturation of 88%. On physical examination, the patient appears drowsy, crackles are heard on chest auscultation bilaterally, and the heart sounds are irregular. A chest X-ray shows hyperinflation of the lungs bilaterally, and the diaphragm is flattened. An ECG is ordered and shown in the accompanying image. Which of the following is the best initial treatment for this patient's arrhythmia?
A 40-year-old woman comes to the physician for a 6-month history of recurrent episodes of chest pain, racing pulse, dizziness, and difficulty breathing. The episodes last up to several minutes. She also reports urinary urgency and two episodes of loss of consciousness followed by spontaneous recovery. There is no personal or family history of serious illness. She does not smoke or drink alcohol. Vitals signs are within normal limits. Cardiopulmonary examination shows no abnormalities. Holter monitoring is performed. ECG recordings during episodes of tachycardia show a QRS duration of 100 ms, regular RR-interval, and absent P waves. Which of the following is the most likely underlying cause of this patient's condition?
A 44-year-old man comes to the emergency department because of persistent palpitations for the past 2 hours. The day before, he was at a wedding, where he drank several glasses of wine and 9–10 vodka cocktails. He has never had similar symptoms before. He is a manager at a software company and has recently had a lot of work-related stress. He is otherwise healthy and takes no medications. His temperature is 36.5°C (97.7°F), pulse is 90/min and irregularly irregular, respirations are 13/min, and his blood pressure is 128/60 mm Hg. Physical examination shows no other abnormalities. An ECG is performed; no P-waves can be identified. Echocardiography shows no valvular abnormalities and normal ventricular function. One hour later, a repeat ECG shows normal P waves followed by narrow QRS complexes. He is still experiencing occasional palpitations. Which of the following is the most appropriate next step in management?
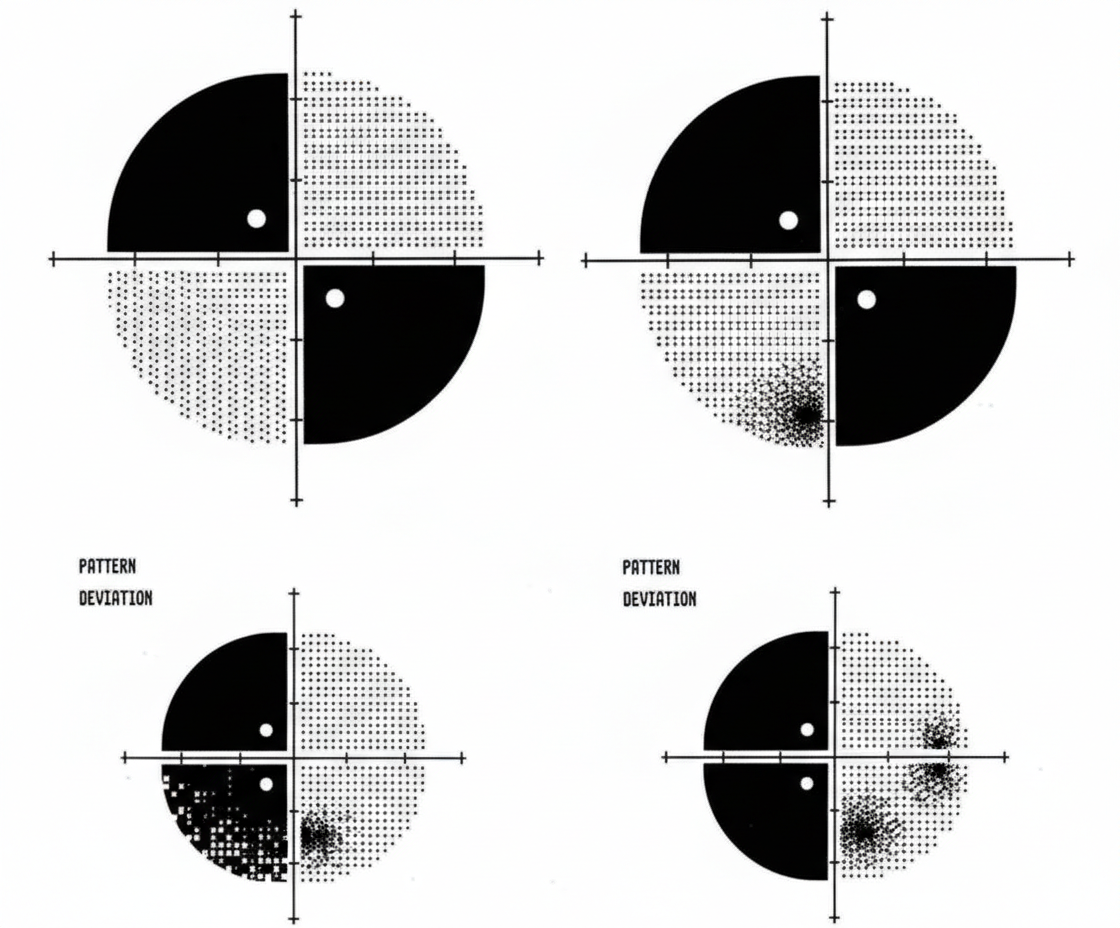
A 62-year-old woman comes to the physician for decreased vision and worsening headaches since this morning. She has hypertension and hypercholesterolemia. Pulse is 119/min and irregular. Current medications include ramipril and atorvastatin. Ocular and funduscopic examination shows no abnormalities. The findings of visual field testing are shown. Which of the following is the most likely cause of this patient's symptoms?
A 54-year-old patient is brought to the emergency department by ambulance with palpitations, lightheadedness, and generalized weakness. He was enjoying the long weekend with his friends at a prolonged destination bachelor's party over the last several days. They all drank a great deal of alcohol. He can't quite recall how much he had to drink but he did not blackout. Past medical history includes hypertension. He takes enalapril daily. His blood pressure is 110/75 mm Hg, pulse 140/min, respiratory rate 14/min, temperature 37.0°C (98.6°F). The patient appears ill and has an irregular pulse. An electrocardiogram is performed (see in the picture). The physician explains to the patient that he has an abnormal heartbeat. If a thrombus were to form in his heart as a complication of this arrhythmia, in which of the following locations would it most likely form?

Practice by Chapter
Basic electrophysiology
Practice Questions
ECG interpretation fundamentals
Practice Questions
Supraventricular tachycardias
Practice Questions
Atrial fibrillation and flutter
Practice Questions
Ventricular arrhythmias
Practice Questions
Bradyarrhythmias and conduction disorders
Practice Questions
Sudden cardiac death
Practice Questions
Antiarrhythmic medications
Practice Questions
Cardioversion and defibrillation
Practice Questions
Pacemakers and ICDs
Practice Questions
Catheter ablation procedures
Practice Questions
Secondary arrhythmias (electrolyte, drug-induced)
Practice Questions
Inherited arrhythmia syndromes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app