
Arrhythmias — MCQs

On this page
A 55-year-old woman visits the clinic after experiencing what she describes as an odd episode of tingling in her fingers and the sensation of smelling sour milk. She denies loss of consciousness, confusion, or incontinence. She also denies a history of head trauma or the ingestion of toxic substances. Past medical history is significant for type 2 diabetes mellitus, which is well controlled with metformin. Her temperature is 36.8°C (98.2°F), the heart rate is 98/min, the respiratory rate is 15/min, the blood pressure is 100/75 mm Hg, and the O2 saturation is 100% on room air. The physical exam, including a full neurologic and cardiac assessment, demonstrates no abnormal findings. Laboratory findings are shown. Brain MRI does not indicate any areas of infarction or hemorrhage. ECG is normal, and EEG is pending. BUN 15 mg/dL pCO2 40 mmHg Creatinine 0.8 mg/dL Glucose 95 mg/dL Serum chloride 103 mmol/L Serum potassium 3.9 mEq/L Serum sodium 140 mEq/L Total calcium 2.3 mmol/L Magnesium 1.7 mEq/L Phosphate 0.9 mmol/L Hemoglobin 14 g/dL Glycosylated hemoglobin 5.5% Total cholesterol 4 mmol/L Bicarbonate (HCO3) 19 mmol/L Urine toxicology screen is negative. What kind of seizure is most likely being described?
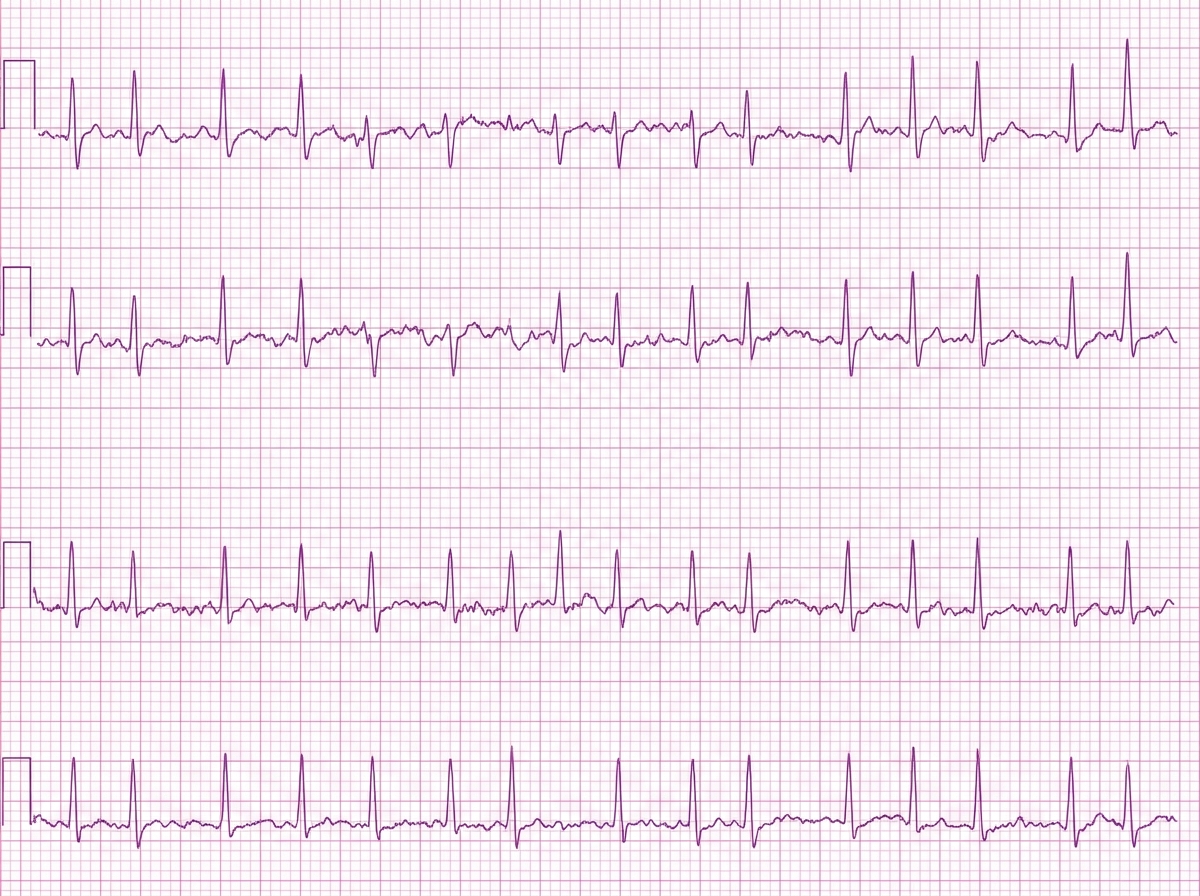
A 62-year-old man with chronic obstructive pulmonary disease presents with palpitations that began at an uncertain time during the past week. His pulse is 140/min and irregular, blood pressure is 116/70 mm Hg, and oxygen saturation is 95% on room air. He has no chest pain, dyspnea, altered mental status, or signs of heart failure. Electrolyte and thyroid-stimulating hormone levels are normal, and echocardiography shows normal left ventricular systolic function. The single-lead rhythm strip shown demonstrates a narrow-complex, irregularly irregular tachycardia without consistently identifiable P waves. He has previously developed severe bronchospasm with a nonselective beta blocker. Which of the following is the most appropriate initial treatment for ventricular rate control?
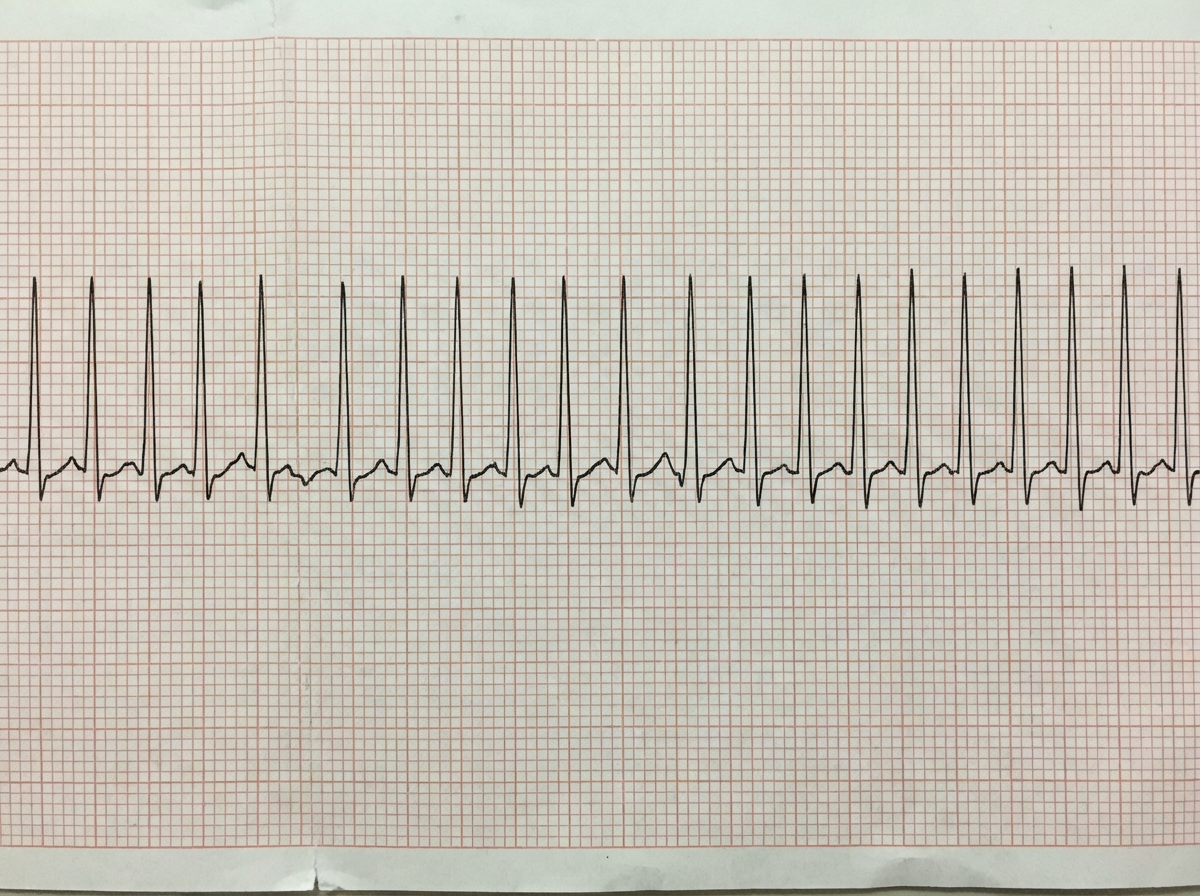
A previously healthy 33-year-old woman comes to the emergency department because she could feel her heart racing intermittently for the last 2 hours. Each episode lasts about 10 minutes. She does not have any chest pain. Her mother died of a heart attack and her father had an angioplasty 3 years ago. She has smoked a half pack of cigarettes daily for 14 years. She drinks one to two beers daily. She appears anxious. Her temperature is 37.6°C (98.1°F), pulse is 160/min, and blood pressure is 104/76 mm Hg. The lungs are clear to auscultation. Cardiac examination shows no murmurs, rubs, or gallops. An ECG is shown. Which of the following is the most appropriate initial step in management?
A 68-year-old woman is brought to the emergency department by her husband because of acute confusion and sudden weakness of her left leg that lasted for about 30 minutes. One hour prior to admission, she was unable to understand words and had slurred speech for about 15 minutes. She has type 2 diabetes mellitus and hypertension. She has smoked 1 pack of cigarettes daily for 30 years. Current medications include metformin and hydrochlorothiazide. Her pulse is 110/min and irregular; blood pressure is 135/84 mmHg. Examination shows cold extremities. There is a mild bruit heard above the left carotid artery. Cardiac examination shows a grade 2/6 late systolic ejection murmur that begins with a midsystolic click. Neurological and mental status examinations show no abnormalities. An ECG shows irregularly spaced QRS complexes with no discernible P waves. Doppler ultrasonography shows mild left carotid artery stenosis. A CT scan and diffusion-weighted MRI of the brain show no abnormalities. Which of the following treatments is most likely to prevent future episodes of neurologic dysfunction in this patient?
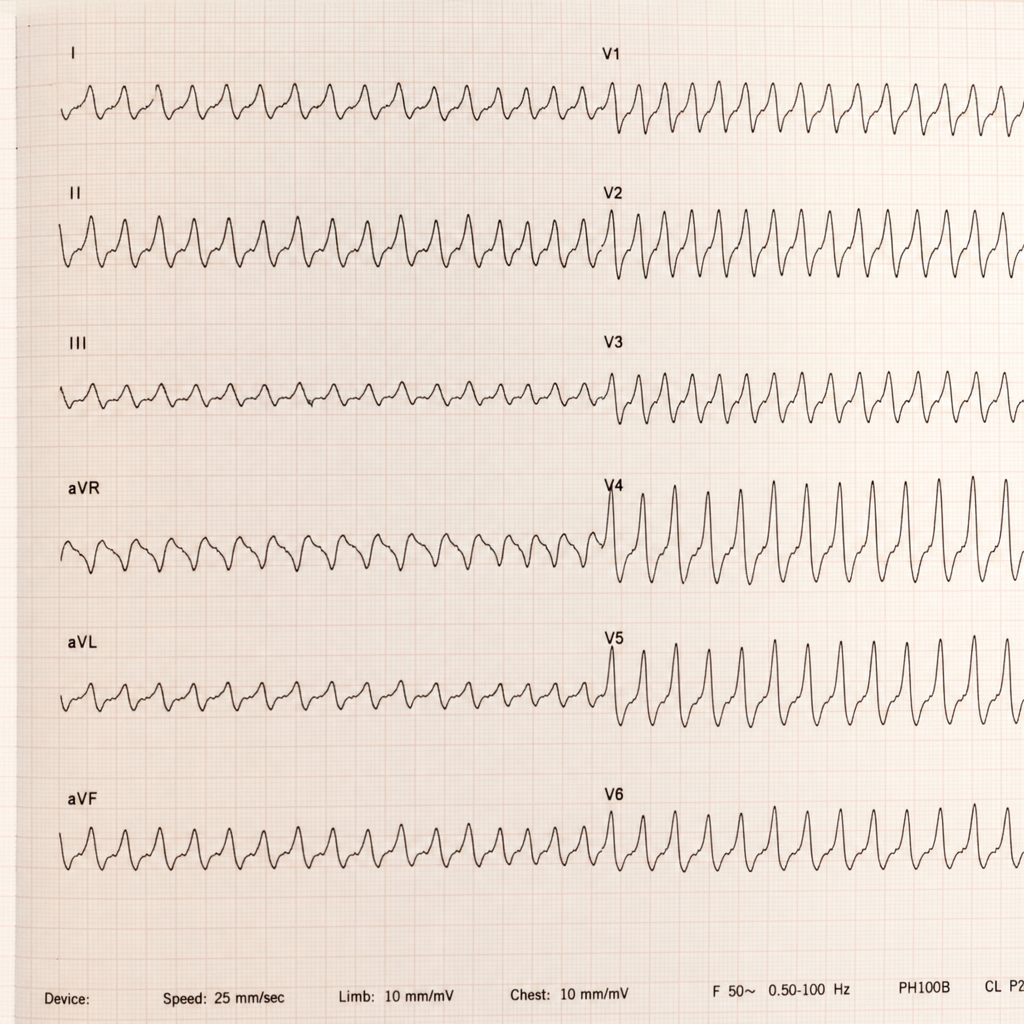
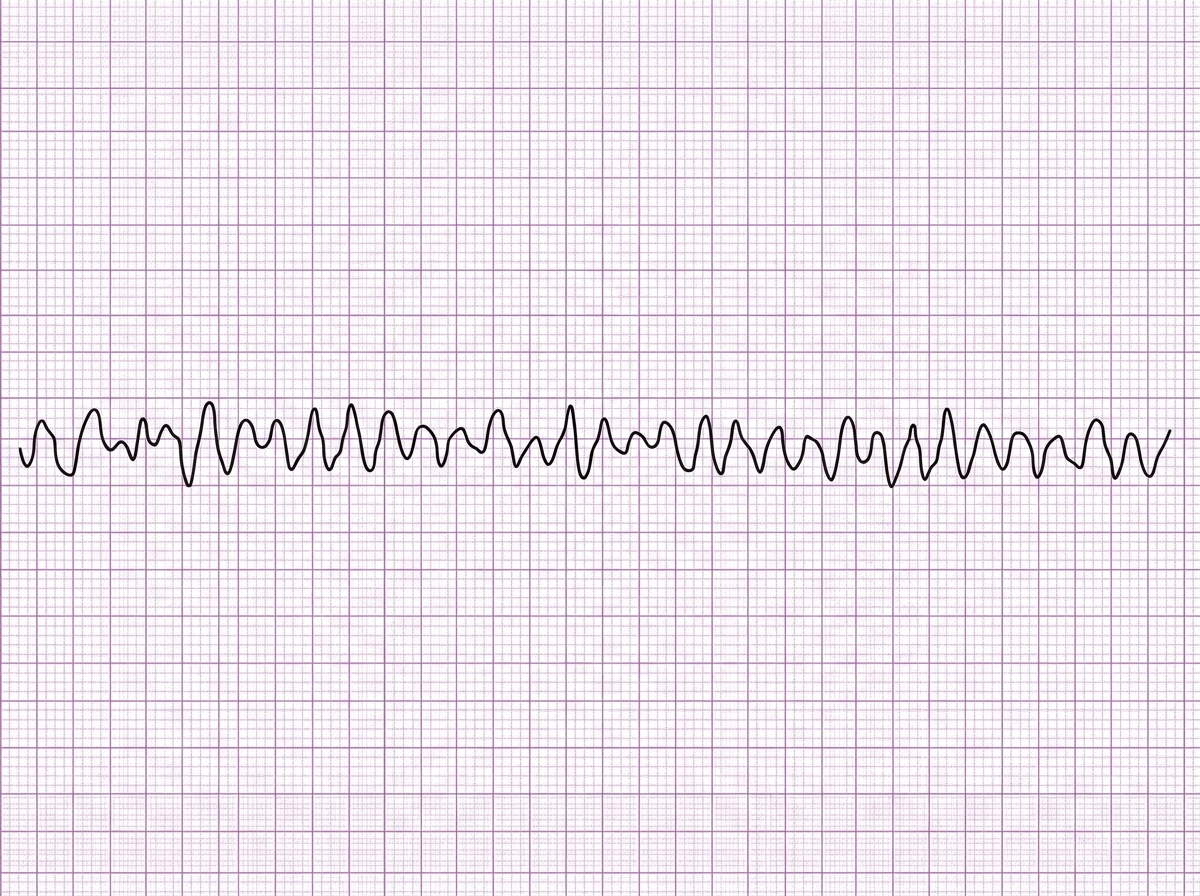
One week after an aortic valve replacement surgery, a 55-year-old man is brought to the emergency room 30 minutes after the onset of severe, sharp chest pain. He appears pale and dyspneic but is alert, oriented, and speaks in full sentences. His temperature is 38°C (100.4°F), pulse is 192/min and thready, respirations are 22/min, and blood pressure is 80/50 mm Hg. Faint rales can be heard in the lower lung fields on both sides on auscultation. There is a midline thoracotomy scar with mild reddening but without warmth or discharge. A portion of an ECG is shown. The pattern remains unchanged after 1 minute. Which of the following is the most appropriate intervention?
A 32-year-old woman is hospitalized after developing an allergic reaction to the contrast medium used for a cerebral angiography. The study was initially ordered as part of the diagnostic approach of a suspected case of pseudotumor cerebri. Her medical history is unremarkable. On physical examination she has stable vital signs, a diffuse maculopapular rash over her neck and chest, and a mild fever. She is started on hydrocortisone and monitored for the next 8 hours. After the monitoring period, a laboratory test shows significant azotemia. The patient complains of generalized weakness and palpitations. Tall-peaked T waves are observed on ECG. Which of the following explains this clinical manifestation?
A 42-year-old woman comes to the physician because of a 5-day history of intermittent palpitations. She has no history of syncope or chest pain. She had similar symptoms 1 year ago and following workup has been treated with daily flecainide since then. She drinks one to two glasses of wine on the weekends. She does not smoke. Her pulse is 71/min and her blood pressure is 134/72 mm Hg. A complete blood count shows no abnormalities. Serum creatinine, electrolytes, and TSH are within normal limits. An ECG is shown. Ablation near which of the following sites would be most appropriate for long-term management of this patient's condition?
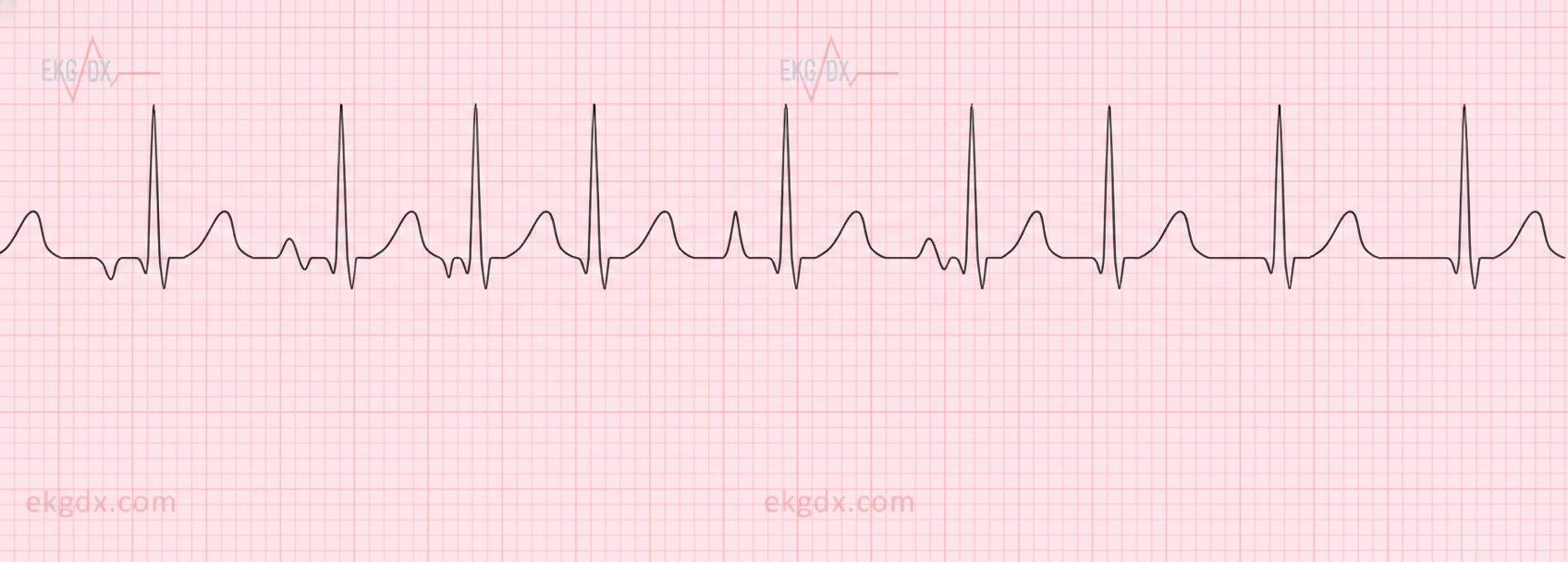
A 54-year-old woman comes to the emergency department because of two episodes of bright red blood per rectum within the past day. She has a history of migraine, which is treated prophylactically with verapamil. She appears well and is hemodynamically stable. Cardiac exam reveals a regular heart rate without any murmurs or gallops. Lungs are clear to auscultation. Her abdomen is mildly tender without rebound or guarding. Digital rectal examination shows fresh blood on the glove. Laboratory studies show: Hemoglobin 10.4 g/dL Leukocyte count 5,000/mm3 Platelet count 175,000/mm3 Partial thromboplastin time 35 seconds Serum Na+ 140 mEq/L K+ 3.7 mEq/L Cl- 101 mEq/L HCO3- 25 mEq/L Mg2+ 1.8 mEq/L A routine ECG shows a heart rate of 75/min, a normal axis, PR interval of 280 ms, QRS interval of 80 ms with a QRS complex following each p wave, and no evidence of ischemic changes. Which of the following is the most appropriate next step in management with respect to this patient's cardiovascular workup?
A 60-year-old male presents with palpitations. He reports drinking many glasses of wine over several hours at a family wedding the previous evening. An EKG reveals absent P waves and irregularly irregular rhythm. He does not take any medications. Which is most likely responsible for the patient’s symptoms?
A 66-year-old man presents to the emergency department with a 3-hour history of crushing chest pain radiating to the left shoulder and neck. Patient states that the pain began suddenly when he was taking a walk around the block and has not improved with rest. He also mentions difficulty breathing and prefers to sit leaning forward. He denies ever having similar symptoms before. Past medical history is significant for hypertension, diagnosed 10 years ago, and hyperlipidemia diagnosed 8 years ago. Current medications are atorvastatin. Patient is also prescribed hydrochlorothiazide as an antihypertensive but is not compliant because he says it makes him urinate too often. Vitals show a blood pressure of 152/90 mm Hg, pulse of 106/min, respirations of 22/min and oxygen saturation of 97% on room air. On physical exam, patient is profusely diaphoretic and hunched over in distress. Cardiac exam is unremarkable and lungs are clear to auscultation. During your examination, the patient suddenly becomes unresponsive and a pulse cannot be palpated. A stat ECG shows the following (see image). Which of the following is the next best step in management?
Practice by Chapter
Basic electrophysiology
Practice Questions
ECG interpretation fundamentals
Practice Questions
Supraventricular tachycardias
Practice Questions
Atrial fibrillation and flutter
Practice Questions
Ventricular arrhythmias
Practice Questions
Bradyarrhythmias and conduction disorders
Practice Questions
Sudden cardiac death
Practice Questions
Antiarrhythmic medications
Practice Questions
Cardioversion and defibrillation
Practice Questions
Pacemakers and ICDs
Practice Questions
Catheter ablation procedures
Practice Questions
Secondary arrhythmias (electrolyte, drug-induced)
Practice Questions
Inherited arrhythmia syndromes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app