
Arrhythmias — MCQs

On this page
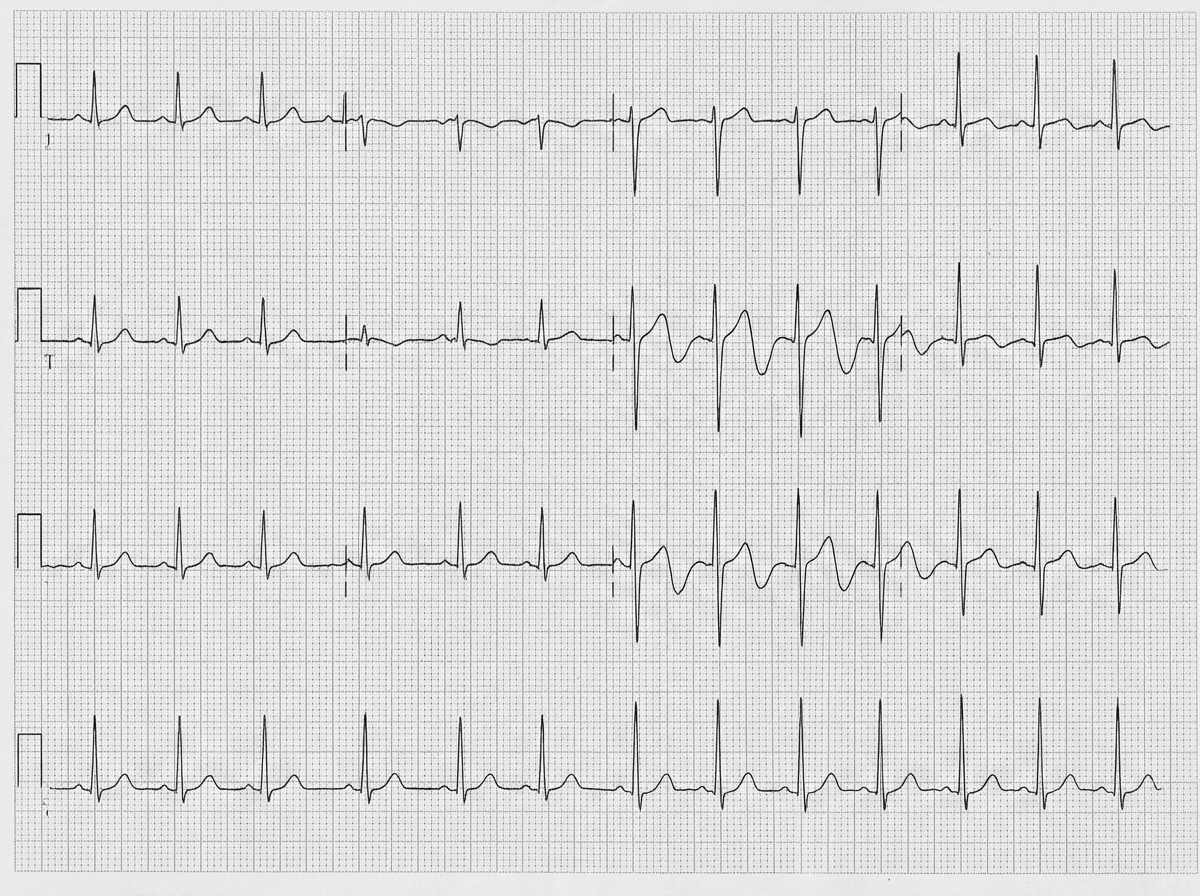
Two days after an uncomplicated laparoscopic abdominal hernia repair, a 46-year-old man is evaluated for palpitations. He has a history of hypertension, type 2 diabetes mellitus, and a ventricular septal defect that closed spontaneously as a child. His father has coronary artery disease. Prior to admission, his only medications were hydrochlorothiazide and metformin. He currently also takes hydromorphone/acetaminophen for mild postoperative pain. He is 180 cm (5 ft 11 in) tall and weighs 100 kg (220 lb); BMI is 30.7 kg/m2. His temperature is 37.0°C (99°F), blood pressure is 139/85 mmHg, pulse is 75/min and irregular, and respirations are 14/min. Cardiopulmonary examination shows a normal S1 and S2 without murmurs and clear lung fields. The abdominal incisions are clean, dry, and intact. There is mild tenderness to palpation over the lower quadrants. An electrocardiogram is obtained and shown below. Which of the following is the most likely cause of this patient's ECG findings?
A 30-year-old man presents with progressive muscle weakness for the past 6 hours. He says he had significant bilateral ankle pain which onset shortly after completing a triathlon earlier in the day. Then, he says he awoke this morning with bilateral upper and lower extremity weakness, which has progressively worsened. He has no significant past medical history and takes no current medication. The vital signs include: temperature 37.0℃ (98.6℉), pulse 66/min, respiratory rate 21/min, and blood pressure 132/83 mm Hg. On physical examination, the patient has diffuse moderate to severe muscle pain on palpation. His strength is 5 out of 5, and deep tendon reflexes are 2+ in the upper and lower extremities bilaterally. Laboratory findings are significant for the following: Laboratory test Sodium 141 mEq/L Potassium 6.3 mEq/L Chloride 103 mEq/L Bicarbonate 25 mEq/L Blood urea nitrogen (BUN) 31 mg/dL Creatinine 6.1 mg/dL BUN/Creatinine 5.0 Glucose (fasting) 80 mg/dL Calcium 6.3 mg/dL Serum creatine kinase (CK) 90 mcg/L (ref: 10–120 mcg/L) Which of the following is the next best step in the management of this patient?
A 40-year-old man is brought to the emergency department 20 minutes after his wife found him unconscious on the bathroom floor. On arrival, he is conscious and alert. He remembers having palpitations and feeling lightheaded and short of breath before losing consciousness. He takes captopril for hypertension and glyburide for type 2 diabetes mellitus. His vitals are within normal limits. Physical examination shows no abnormalities. Random serum glucose concentration is 85 mg/dL. An ECG shows a short PR interval and a wide QRS complex with initial slurring. Transthoracic echocardiography reveals normal echocardiographic findings with normal left ventricular systolic function. Which of the following is the most likely underlying cause of this patient's findings?
A 23-year-old man comes to the physician because of a 1-year history of episodic shortness of breath. Physical examination shows no abnormalities. Laboratory studies show elevated serum IgE levels. Microscopic examination of the sputum shows eosinophilic, hexagonal, double-pointed crystals. A methacholine challenge test is positive. Exposure to which of the following is most likely responsible for this patient's condition?
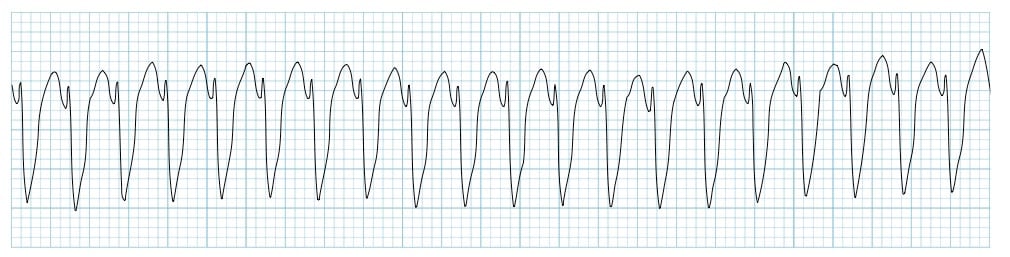
A 72-year-old man is taken to the emergency room after losing consciousness. According to his wife, he suddenly complained of fluttering in his chest, lightheadedness, and profuse sweating while walking to the grocery store. He then turned gray, lost consciousness, and collapsed onto the ground. His medical history is significant for a prior anterior wall myocardial infarction 2 years ago that was complicated by severe left ventricular systolic dysfunction. His blood pressure was 80/50 mm Hg before he became pulseless, the temperature is 36.7°C (98.0°F), and the carotid pulse is not palpable. An ECG was obtained and the results are shown in the picture. Cardiopulmonary resuscitation is initiated and the patient is cardioverted to sinus rhythm with an external defibrillator. The patient regains consciousness and states there was no antecedent chest discomfort. Cardiac enzymes are negative and serum electrolytes are normal. Which of the following is the best next step for this patient?
A 55-year-old woman presents to the physician with repeated episodes of dizziness for the last 3 months, which are triggered by rising from a supine position and by lying down. The episodes are sudden and usually last for less than 30 seconds. During the episode, she feels as if she is suddenly thrown into a rolling spin. She has no symptoms in the period between episodes. The patient denies having headaches, vomiting, deafness, ear discharge or ear pain. There is no history of a known medical disorder or prolonged consumption of a specific drug. The vital signs are within normal limits. On physical examination, when the physician asks the woman to turn her head 45° to the right, and then to rapidly move from the sitting to the supine position, self-limited rotatory nystagmus is observed following her return to the sitting position. The rest of the neurological examination is normal. Which of the following is the treatment of choice for the condition of this patient?
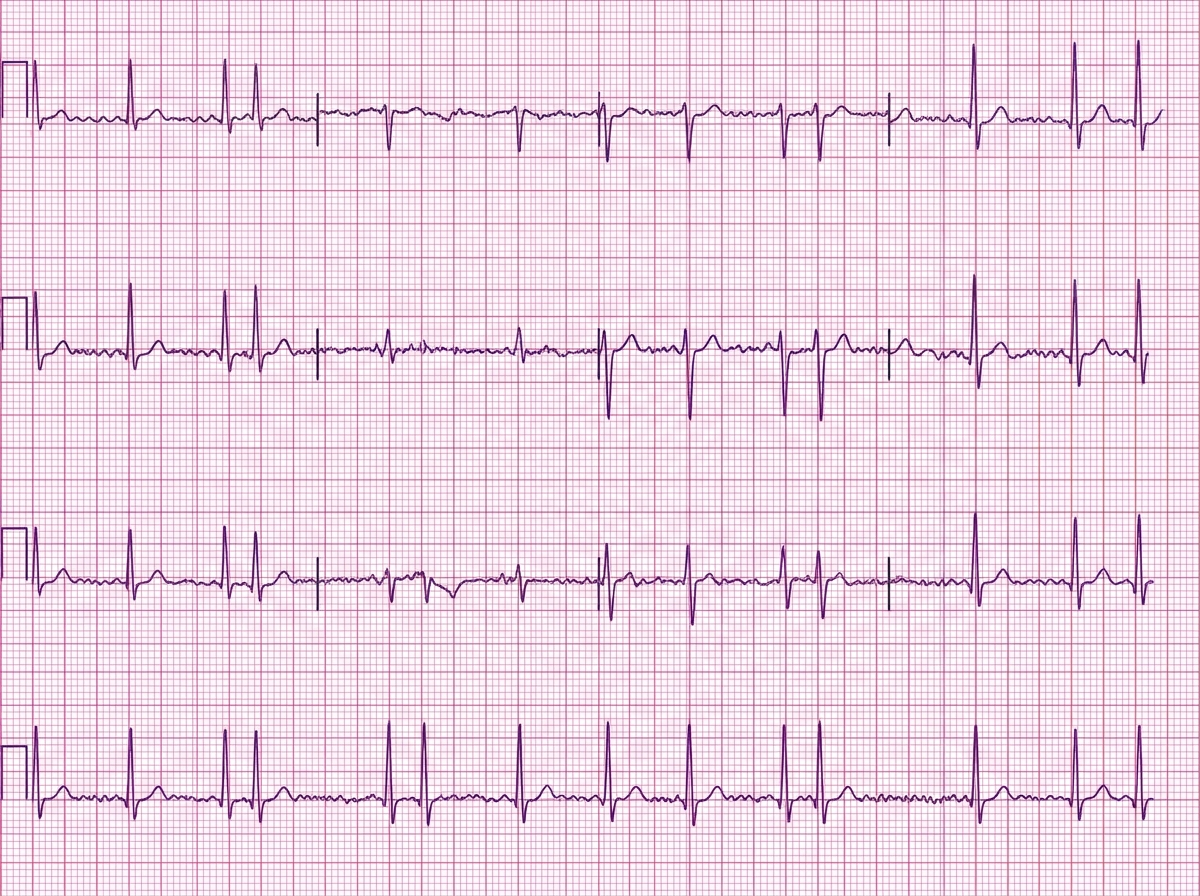
A 77-year-old man presents to the emergency department complaining of feeling like "his heart was racing" for the last 8 days. He denies any chest pain, dizziness, or fainting but complains of fatigue, difficulty breathing with exertion, and swelling of his legs bilaterally for the last 2 weeks. He has had hypertension for the last 25 years. He has a long history of heavy alcohol consumption but denies smoking. His blood pressure is 145/70 mm Hg and the pulse is irregular at the rate of 110/min. On examination of his lower limbs, mild pitting edema is noted of his ankles bilaterally. On cardiac auscultation, heart sounds are irregular. Bibasilar crackles are heard with auscultation of the lungs. An ECG is ordered and the result is shown in the image. Transesophageal echocardiography shows a reduced ejection fraction of 32% and dilatation of all chambers of the heart without any obvious intracardiac thrombus. Which of the following is the optimal therapy for this patient?
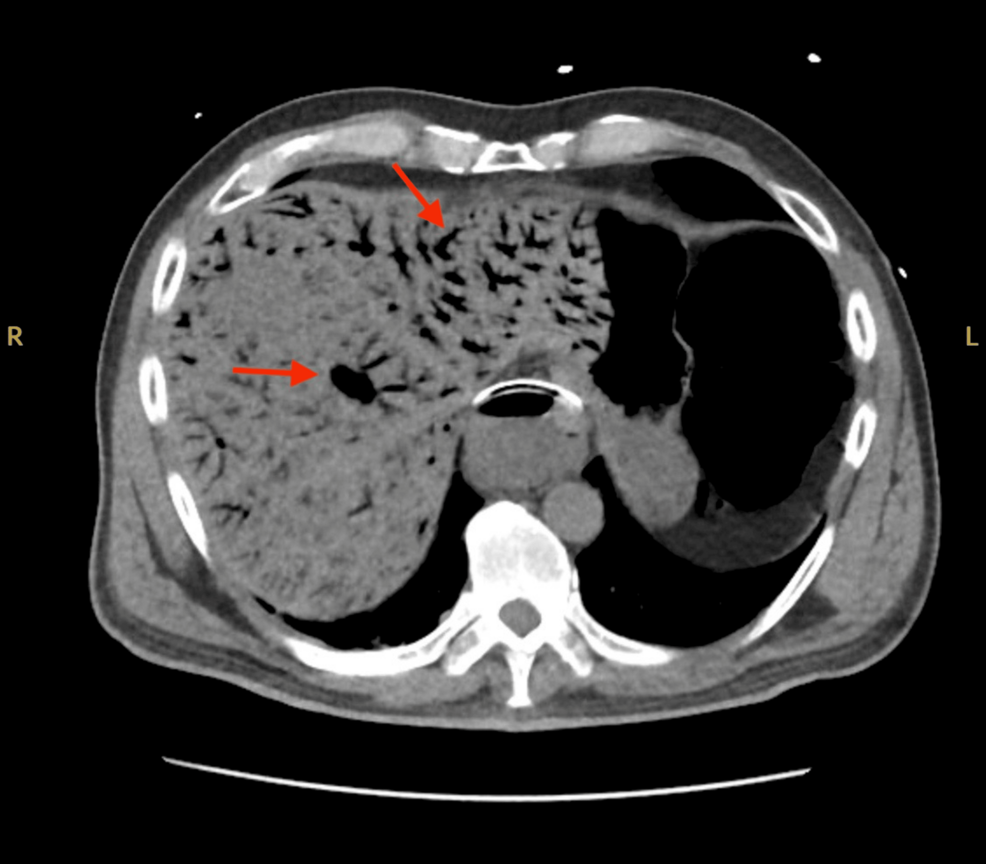
A 76-year-old woman with a history of hypertension and type 2 diabetes mellitus is brought to the emergency department 60 minutes after the acute onset of left-sided abdominal pain and nausea with vomiting. Three weeks ago, she underwent emergency surgical revascularization for acute left lower extremity ischemia. Physical examination shows left upper quadrant tenderness without rebound or guarding. Serum studies show an elevated lactate dehydrogenase level. Laboratory studies, including a complete blood count, basic metabolic panel, and hepatic panel, are otherwise unremarkable. A transverse section of a CT scan of the abdomen is shown. Further evaluation is most likely to show which of the following?
A 21-year-old woman presents with palpitations and anxiety. She had a recent outpatient ECG that was suggestive of supraventricular tachycardia, but her previous physician failed to find any underlying disease. No other significant past medical history. Her vital signs include blood pressure 102/65 mm Hg, pulse 120/min, respiratory rate 17/min, and temperature 36.5℃ (97.7℉). Electrophysiological studies reveal an atrioventricular nodal reentrant tachycardia. The patient refuses an ablation procedure so it is decided to perform synchronized cardioversion with consequent ongoing management with verapamil. Which of the following ECG features should be monitored in this patient during treatment?
A previously healthy 66-year-old woman comes to the physician because of a 3-day history of fever, cough, and right-sided chest pain. Her temperature is 38.8°C (101.8°F) and respirations are 24/min. Physical examination shows dullness to percussion, increased tactile fremitus, and egophony in the right lower lung field. The remainder of the examination shows no abnormalities. Which of the following is the most likely cause of these findings?
Practice by Chapter
Basic electrophysiology
Practice Questions
ECG interpretation fundamentals
Practice Questions
Supraventricular tachycardias
Practice Questions
Atrial fibrillation and flutter
Practice Questions
Ventricular arrhythmias
Practice Questions
Bradyarrhythmias and conduction disorders
Practice Questions
Sudden cardiac death
Practice Questions
Antiarrhythmic medications
Practice Questions
Cardioversion and defibrillation
Practice Questions
Pacemakers and ICDs
Practice Questions
Catheter ablation procedures
Practice Questions
Secondary arrhythmias (electrolyte, drug-induced)
Practice Questions
Inherited arrhythmia syndromes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app