
Arrhythmias — MCQs

On this page
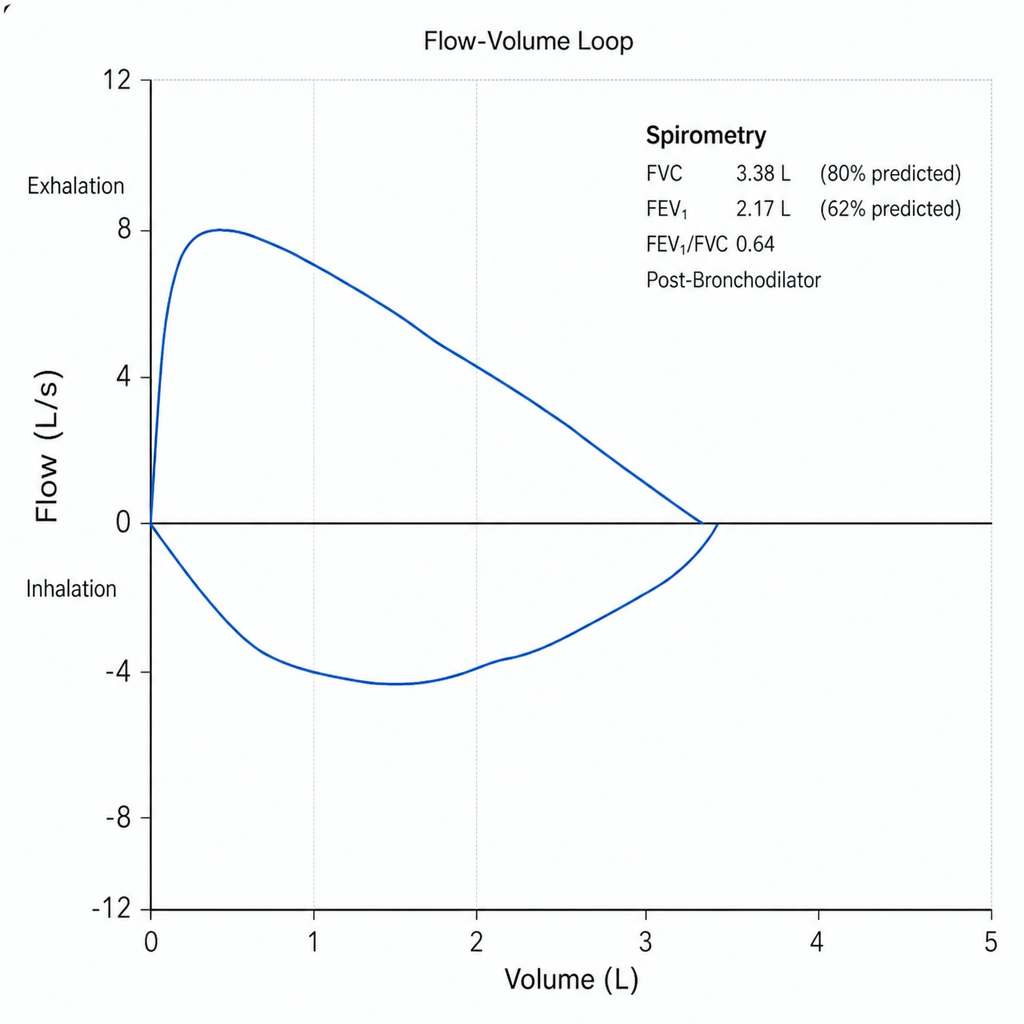
A 58-year-old man with a 40 pack-year smoking history presents with progressive dyspnea over 8 months, a chronic productive cough, and two hospitalizations for respiratory infections in the past year. He uses albuterol as needed with partial relief. Spirometry is performed and the flow-volume loop is shown below. Post-bronchodilator FEV₁/FVC is 0.64 and FEV₁ is 62% of predicted. Which of the following best describes the physiologic pattern and the most appropriate escalation of maintenance therapy?
Match the following A. Atrial fibrillation B. Atrial flutter C. PSVT D. Ventricular tachycardia
A patient with a history of hypertension presents with atrial fibrillation, shortness of breath, and bilateral basal crackles on auscultation. Which of the following would be the least important in the management of this patient?
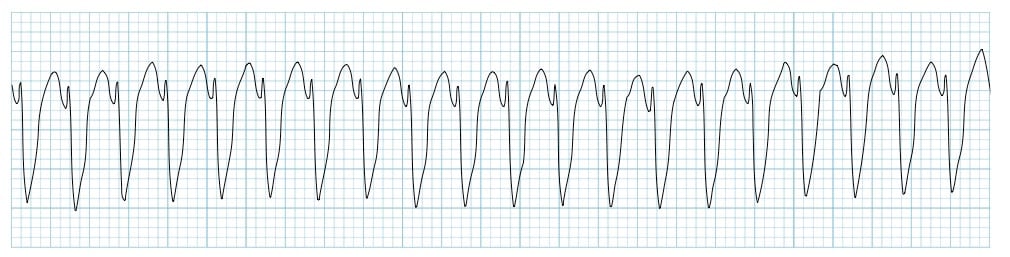
A patient is pulseless with the following rhythm shown in the ECG. What is the next best step in management?
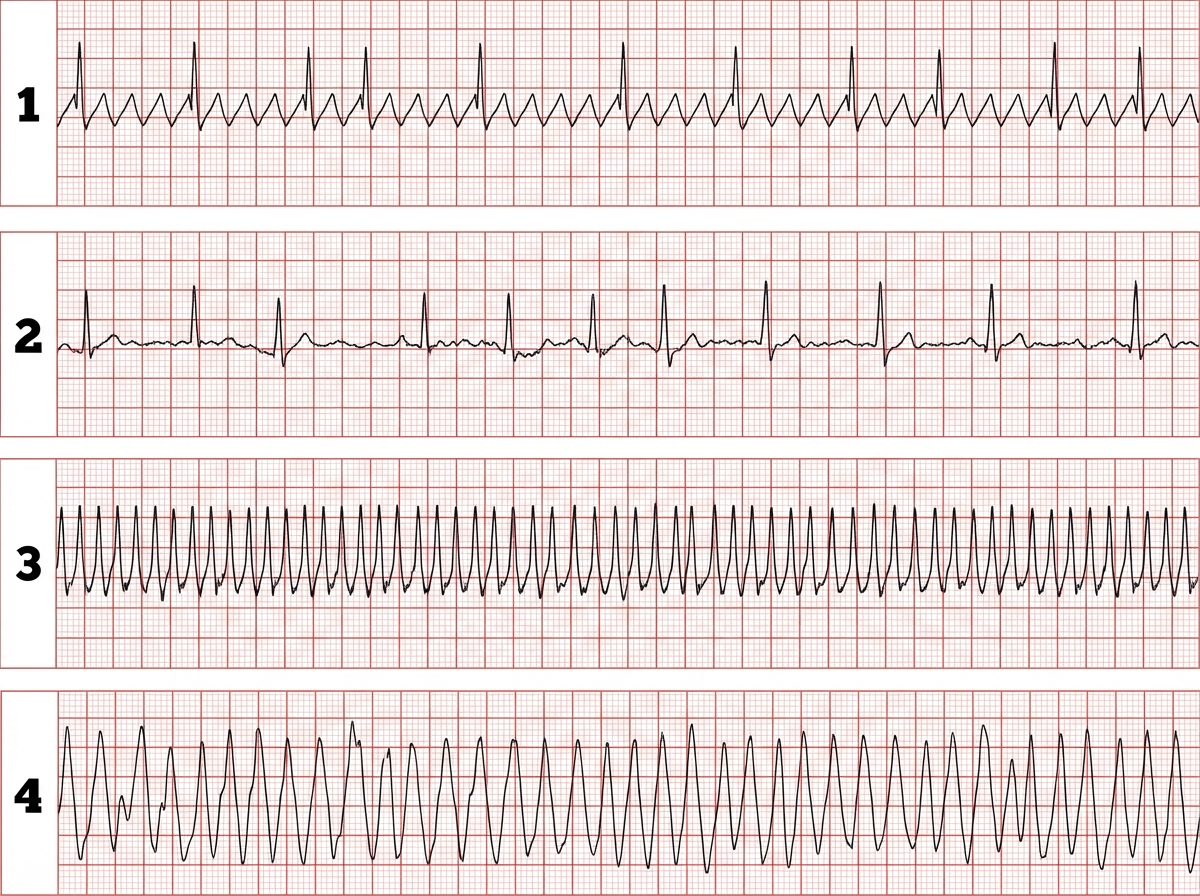
Match the following ECG findings (1-4) with their corresponding arrhythmias (A-D): 1. Sawtooth pattern in leads II, III, aVF with regular ventricular response 2. Irregularly irregular rhythm with absent P waves 3. Narrow QRS tachycardia with abrupt onset/termination 4. Wide QRS tachycardia with AV dissociation A. Atrial fibrillation B. PSVT (Paroxysmal Supraventricular Tachycardia) C. Atrial flutter D. Ventricular tachycardia What is the correct matching?
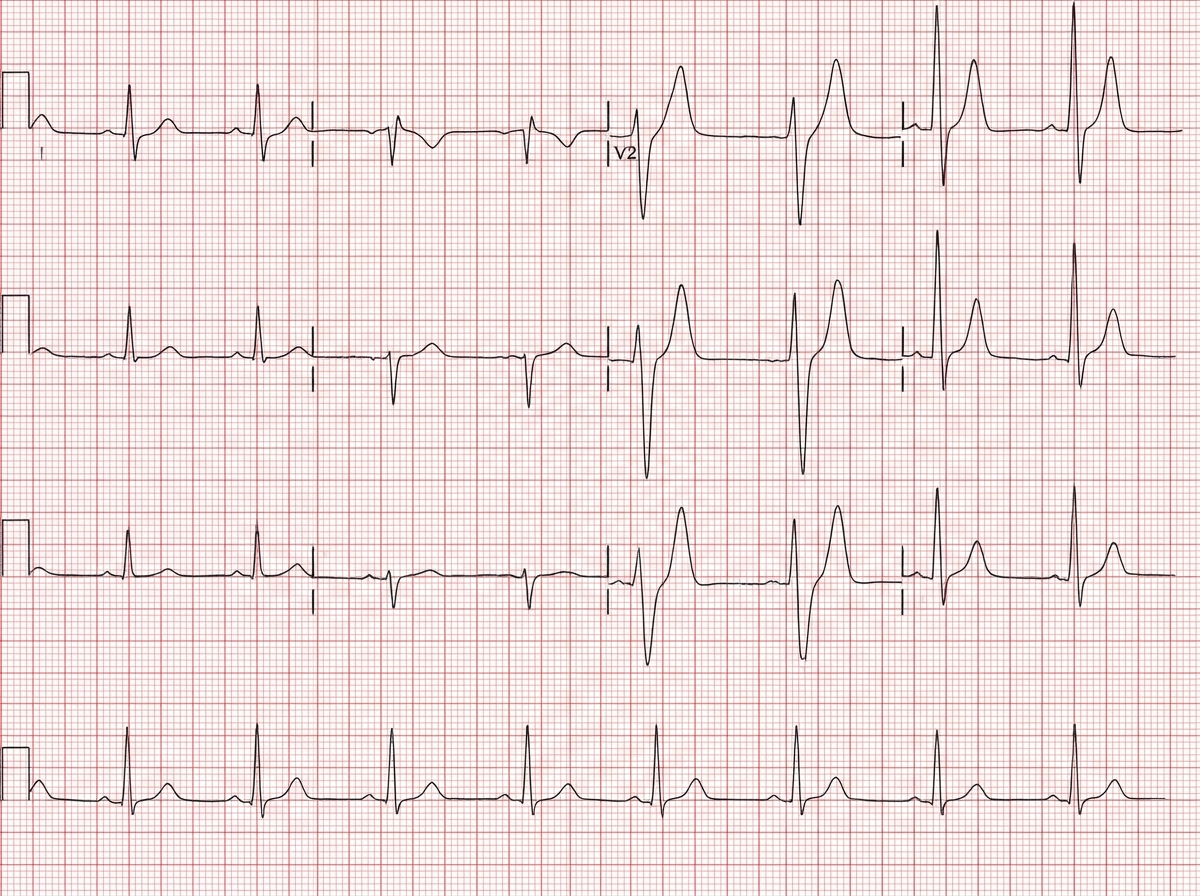
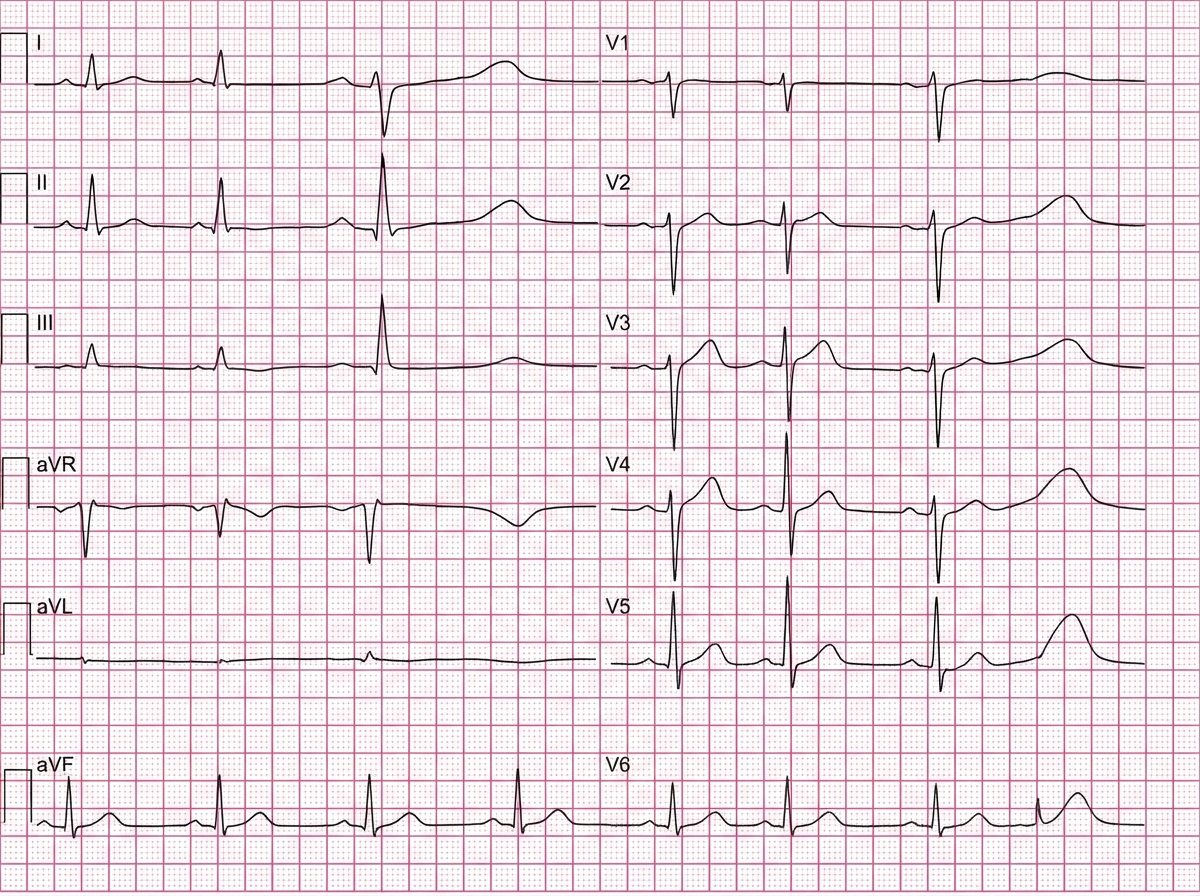
A 45-year-old male is brought into the emergency department by emergency medical services. The patient has a history of substance abuse and was found down in his apartment lying on his right arm. He was last seen 24 hours earlier by his mother who lives in the same building. He is disoriented and unable to answer any questions. His vitals are HR 48, T 97.6, RR 18, BP 100/75. You decide to obtain an EKG as shown in Figure 1. Which of the following is most likely the cause of this patient's EKG results?
A previously healthy 22-year-old woman comes to the emergency department because of several episodes of palpitations that began a couple of days ago. The palpitations are intermittent in nature, with each episode lasting 5–10 seconds. She states that during each episode she feels as if her heart is going to “spin out of control.” She has recently been staying up late to study for her final examinations. She does not drink alcohol or use illicit drugs. She appears anxious. Her temperature is 37°C (98.6°F), pulse is 75/min, and blood pressure is 110/75 mm Hg. Physical examination shows no abnormalities. An ECG is shown. Which of the following is the most appropriate next step in management?
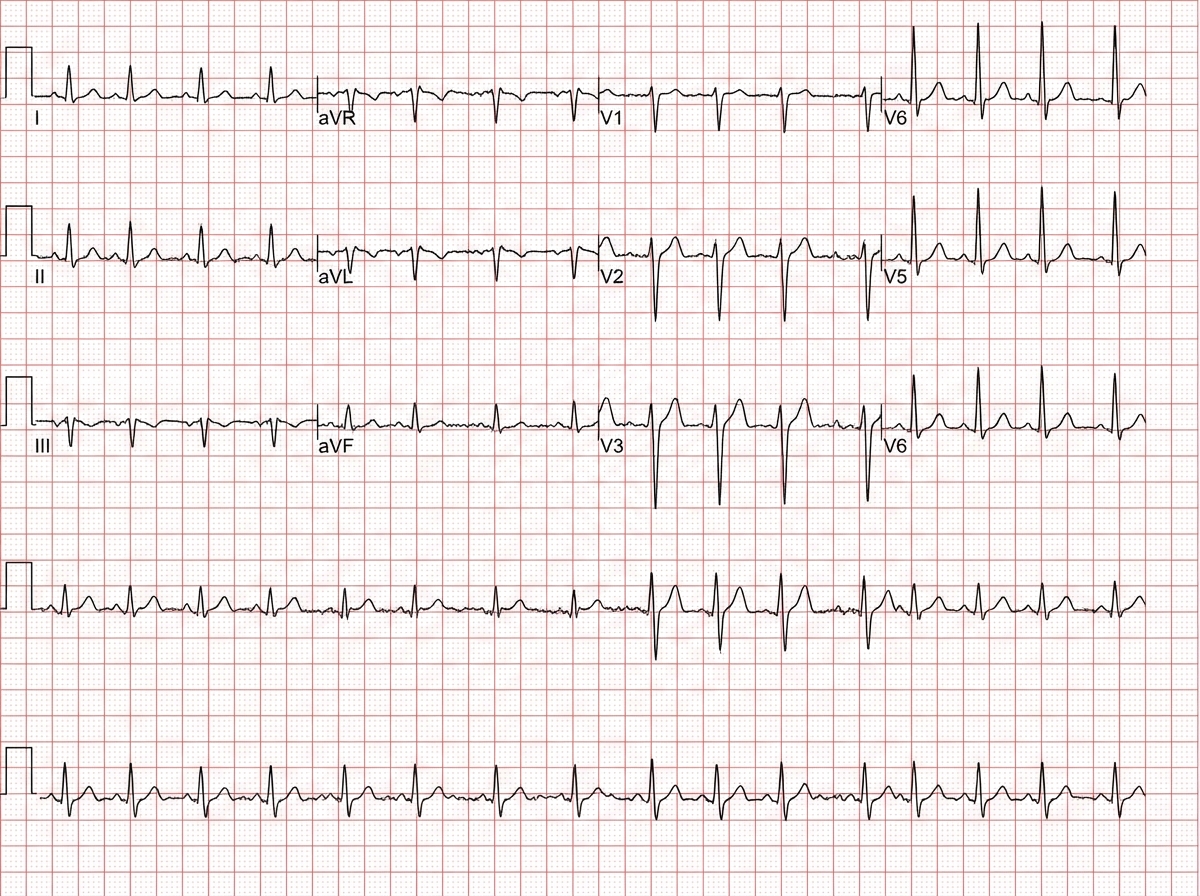
A 23-year-old patient who has recently found out she was pregnant presents to her physician for her initial prenatal visit. The estimated gestational age is 10 weeks. Currently, the patient complains of recurrent palpitations. She is gravida 1 para 0 with no history of any major diseases. On examination, the blood pressure is 110/60 mm Hg heart rate, heart rate 94/min irregular, respiratory rate 12/min, and temperature 36.4°C (97.5°F). Her examination is significant for an opening snap before S2 and diastolic decrescendo 3/6 murmur best heard at the apex. No venous jugular distension or peripheral edema is noted. The patient’s electrocardiogram (ECG) is shown in the image. Cardiac ultrasound reveals the following parameters: left ventricular wall thickness 0.4 cm, septal thickness 1 cm, right ventricular wall thickness 0.5 cm, mitral valve area 2.2 cm2, and tricuspid valve area 4.1 cm2. Which of the following statements regarding this patient’s management is correct?
A 52-year-old woman presents with decreased exercise tolerance and difficulty breathing on exertion and while sleeping at night. She says that she requires 2 pillows to sleep at night to alleviate her shortness of breath. These symptoms started 6 months ago and are gradually increasing in severity. She does not have any chronic health problems. She has smoked 15 cigarettes per day for the past 20 years and drinks alcohol occasionally. Vital signs include: blood pressure 110/70 mm Hg, temperature 36.7°C (98.0°F), and regular pulse 90/min. On physical examination, the first heart sound is loud, and there is a low pitched rumbling murmur best heard at the cardiac apex. This patient is at high risk of developing which of the following complications?
A 63-year-old woman is brought to the emergency department 1 hour after the onset of right-sided weakness. She was eating breakfast when suddenly she could not lift her spoon. She cried out to her husband but her speech was slurred. For the past 4 months, she has been more anxious than usual and felt fatigued. She used to exercise regularly but had to give up her exercise routine 3 months ago because of lightheadedness and shortness of breath with exertion. She has a history of hypertension. She is a tax accountant and has had increased stress at work recently. She takes lisinopril daily and alprazolam as needed. Her temperature is 37.2°C (99.0°F), pulse is 138/min, respirations are 14/min, and blood pressure is 146/86 mm Hg. Her lungs are clear to auscultation bilaterally and she has an S1 with variable intensity. On neurologic examination, she has a right facial droop and 2/5 strength in the right shoulder, elbow, wrist, and fingers. Sensation is diminished in the right face and arm. Further evaluation is most likely to show which of the following?
Practice by Chapter
Basic electrophysiology
Practice Questions
ECG interpretation fundamentals
Practice Questions
Supraventricular tachycardias
Practice Questions
Atrial fibrillation and flutter
Practice Questions
Ventricular arrhythmias
Practice Questions
Bradyarrhythmias and conduction disorders
Practice Questions
Sudden cardiac death
Practice Questions
Antiarrhythmic medications
Practice Questions
Cardioversion and defibrillation
Practice Questions
Pacemakers and ICDs
Practice Questions
Catheter ablation procedures
Practice Questions
Secondary arrhythmias (electrolyte, drug-induced)
Practice Questions
Inherited arrhythmia syndromes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app