
STEMI diagnosis and management — MCQs

A 28-year-old male presents with sharp, stabbing chest pain that worsens when lying flat and improves when sitting forward. He reports a recent viral upper respiratory infection 2 weeks ago. On examination, a friction rub is heard on auscultation. His vital signs are stable. An ECG is most likely to show which of the following findings in this patient?
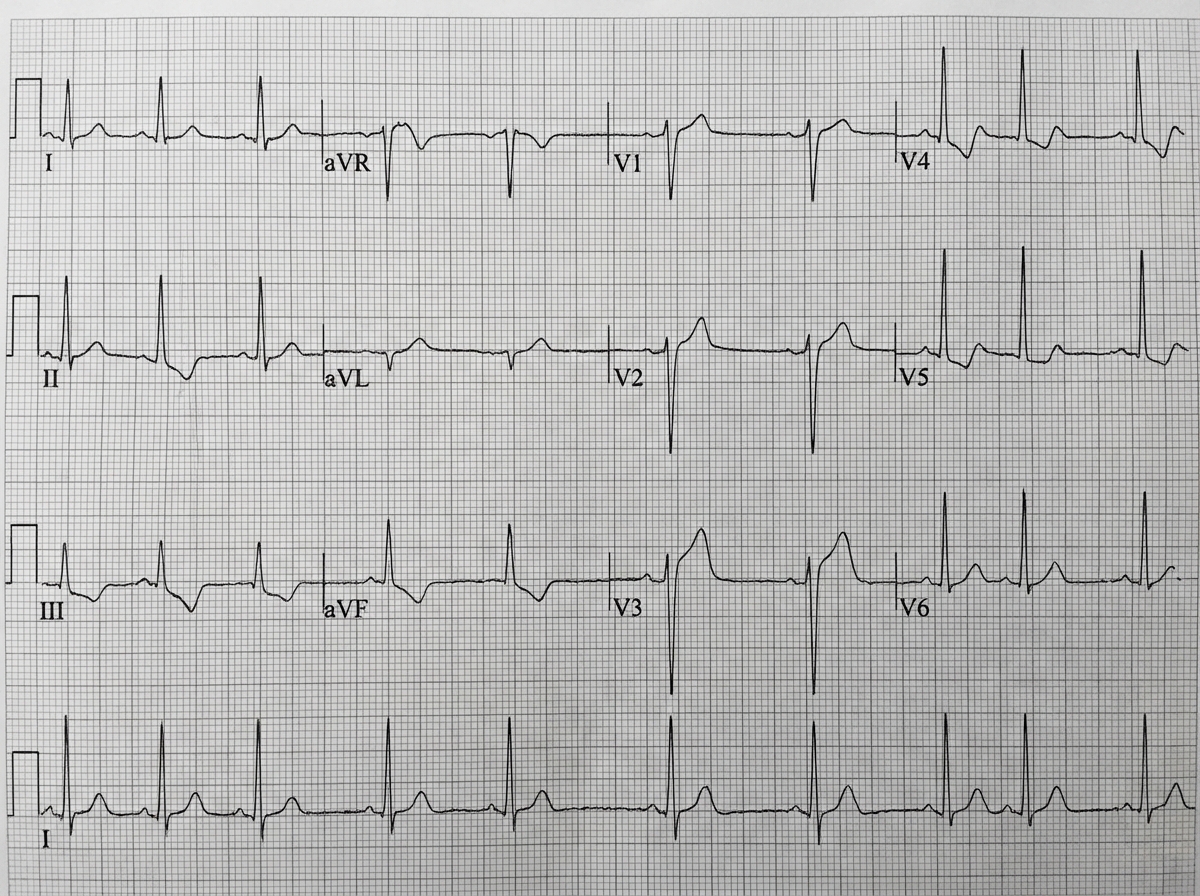
A 71-year-old man develops worsening chest pressure while shoveling snow in the morning. He tells his wife that he has a squeezing pain that is radiating to his jaw and left arm. His wife calls for an ambulance. On the way, he received chewable aspirin and 3 doses of sublingual nitroglycerin with little relief of pain. He has borderline diabetes and essential hypertension. He has smoked 15–20 cigarettes daily for the past 37 years. His blood pressure is 172/91 mm Hg, the heart rate is 111/min and the temperature is 36.7°C (98.0°F). On physical examination in the emergency department, he looks pale, very anxious and diaphoretic. His ECG is shown in the image. Troponin levels are elevated. Which of the following is the best next step in the management of this patient condition?
A 59-year-old woman comes to the physician because of left leg swelling that started after a transcontinental flight. A duplex ultrasound of the left leg shows a noncompressible popliteal vein. A drug is prescribed that inhibits the coagulation cascade. Two weeks later, laboratory studies show: Platelet count 210,000/mm3 Partial thromboplastin time 28 seconds (normal: 25-35) Prothrombin time 12 seconds (normal: 11-13) Thrombin time 15 seconds (control: 15 seconds) Which of the following drugs was most likely prescribed?
A 54-year-old man is brought to the emergency department 1 hour after the sudden onset of shortness of breath, severe chest pain, and sweating. He has hypertension and type 2 diabetes mellitus. He has smoked one pack and a half of cigarettes daily for 20 years. An ECG shows ST-segment elevations in leads II, III, and avF. The next hospital with a cardiac catheterization unit is more than 2 hours away. Reperfusion pharmacotherapy is initiated. Which of the following is the primary mechanism of action of this medication?
A 66-year-old female with hypertension and a recent history of acute ST-elevation myocardial infarction (STEMI) 6 days previous, treated with percutaneous transluminal angioplasty (PTA), presents with sudden onset chest pain, shortness of breath, diaphoresis, and syncope. Vitals are temperature 37°C (98.6°F), blood pressure 80/50 mm Hg, pulse 125/min, respirations 12/min, and oxygen saturation 92% on room air. On physical examination, the patient is pale and unresponsive. Cardiac exam reveals tachycardia and a pronounced holosystolic murmur loudest at the apex and radiates to the back. Lungs are clear to auscultation. Chest X-ray shows cardiomegaly with clear lung fields. ECG is significant for ST elevations in the precordial leads (V2-V4) and low-voltage QRS complexes. Emergency transthoracic echocardiography shows a left ventricular wall motion abnormality along with a significant pericardial effusion. The patient is intubated, and aggressive fluid resuscitation is initiated. What is the next best step in management?
A 52-year-old woman presents to the emergency room complaining of chest pain. She reports a 4-hour history of dull substernal pain radiating to her jaw. Her history is notable for hypertension, diabetes mellitus, and alcohol abuse. She has a 30 pack-year smoking history and takes lisinopril and metformin but has an allergy to aspirin. Her temperature is 99.1°F (37.3°C), blood pressure is 150/90 mmHg, pulse is 120/min, and respirations are 22/min. Physical examination reveals a diaphoretic and distressed woman. An electrocardiogram reveals ST elevations in leads I, aVL, and V5-6. She is admitted with plans for immediate transport to the catheterization lab for stent placement. What is the mechanism of the next medication that should be given to this patient?
A 71-year-old woman with a past medical history of type 2 diabetes, hypercholesterolemia, and hypertension was admitted to the hospital 8 hours ago with substernal chest pain for management of acute non-ST-elevated myocardial infarction (NSTEMI). The ECG findings noted by ST-depressions and T-wave inversions on anterolateral leads, which is also accompanied by elevated cardiac enzymes. Upon diagnosis, management with inhaled oxygen therapy, beta-blockers and aspirin, and low-molecular-weight heparin therapy were initiated, and she was placed on bed rest with continuous electrocardiographic monitoring. Since admission, she required 2 doses of sublingual nitroglycerin for recurrent angina, and the repeat troponin levels continued to rise. Given her risk factors, plans were made for early coronary angiography. The telemetry nurse calls the on-call physician because of her concern with the patient's mild confusion and increasing need for supplemental oxygen. At bedside evaluation, The vital signs include: heart rate 122/min, blood pressure 89/40 mm Hg, and the pulse oximetry is 91% on 6L of oxygen by nasal cannula. The telemetry and a repeat ECG show sinus tachycardia. She is breathing rapidly, appears confused, and complains of shortness of breath. On physical exam, the skin is cool and clammy and appears pale and dull. She has diffuse bilateral pulmonary crackles, and an S3 gallop is noted on chest auscultation with no new murmurs. She has jugular venous distention to the jaw-line, rapid and faint radial pulses, and 1+ dependent edema. She is immediately transferred to the intensive care unit for respiratory support and precautions for airway security. The bedside sonography shows abnormal hypodynamic anterior wall movement and an ejection fraction of 20%, but no evidence of mitral regurgitation or ventricular shunt. The chest X-ray demonstrates cephalization of pulmonary veins and pulmonary edema. What is the most appropriate next step in the stabilization of this patient?
A 70-year-old man is brought to the emergency room with complaints of severe substernal chest pain for the last hour. The pain started suddenly, and the patient describes the pain as “going into the shoulder”. The patient took aspirin at home and has been given multiple doses of sublingual nitroglycerin, but the pain has not subsided. He has a blood pressure of 112/84 mm Hg, the pulse is 63/min, the respiratory rate is 18/min, and the temperature is 36.9°C (98.0°F). Cardiac auscultation reveals normal S1 and S2 sounds, however, an additional S4 sound is heard. The patient is sweating profusely, and the lungs are clear to auscultation. No jugular venous distension or pedal edema is observed. His initial ECG shows ST elevation in leads II, III, and aVF. Which of the following will likely have the most benefit in this patient?
A 70-year-old man presents to the emergency department with severe substernal chest pain of one hour’s duration. The patient was taking a morning walk when the onset of pain led him to seek care. His past medical history includes coronary artery disease, hyperlipidemia, and hypertension. Medications include aspirin, losartan, and atorvastatin. An electrocardiogram reveals ST elevations in the inferior leads II, III, and avF as well as in leads V5 and V6. The ST elevations found in leads V5-V6 are most indicative of pathology in which of the following areas of the heart?
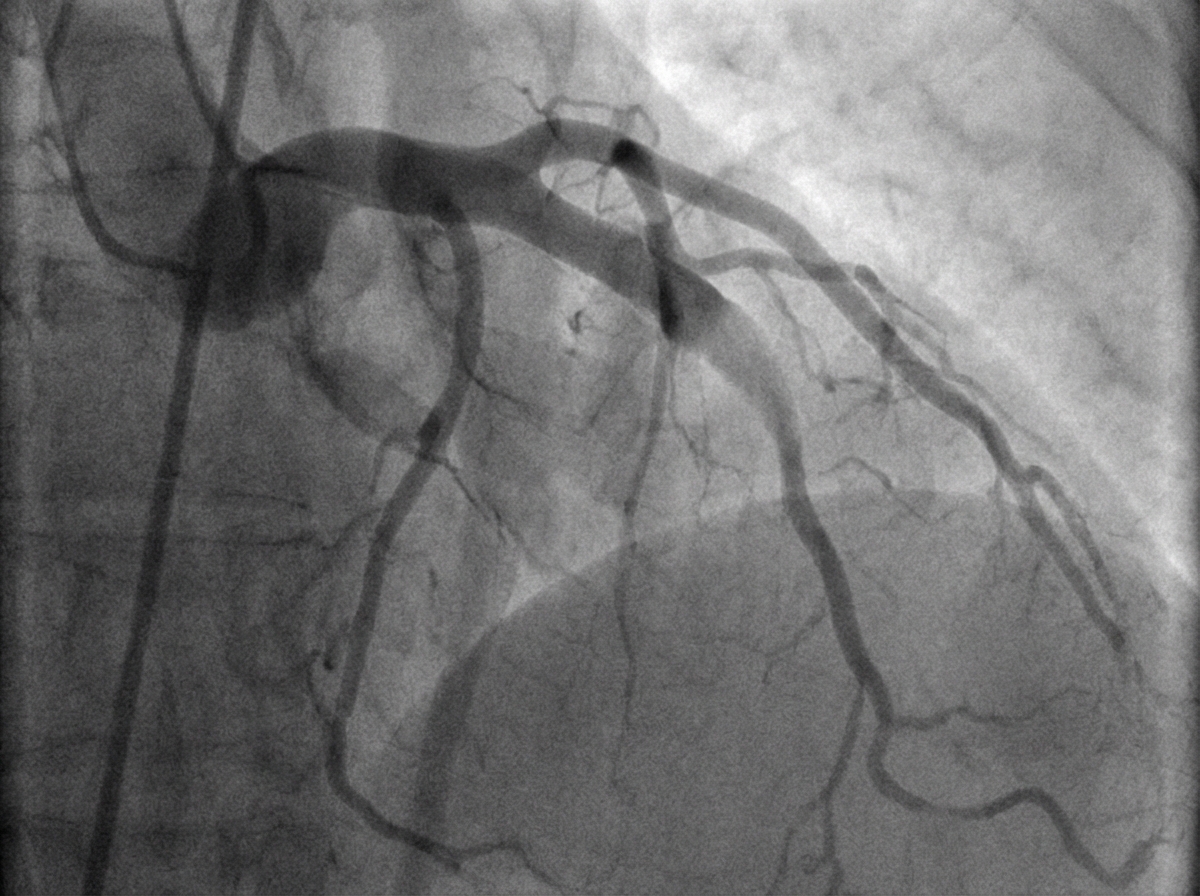
A 54-year-old woman is brought to the emergency department because of a 2-hour history of nausea and retrosternal chest pain. She has a 15-year history of type 2 diabetes mellitus. Her current medications include atorvastatin, metformin, and lisinopril. She is diaphoretic. Her serum troponin level is 3.0 ng/mL (N: < 0.04). She undergoes cardiac catheterization. A photograph of coronary angiography performed prior to percutaneous coronary intervention is shown. An acute infarct associated with the finding on angiography is most likely to manifest with ST elevations in which of the following leads on ECG?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app