
ACS — MCQs

On this page
A 65-year-old man presents to the emergency room with chest pain. Coronary angiography reveals significant stenosis of the left anterior descending (LAD) artery. Which of the following factors best predicts the risk of myocardial necrosis in this clinical setting?
A 73-year-old man presents to the outpatient clinic complaining of chest pain with exertion. He states that resting for a few minutes usually resolves the chest pain. Currently, he takes 81 mg of aspirin daily. He has a blood pressure of 127/85 mm Hg and heart rate of 75/min. Physical examination reveals regular heart sounds and clear lung sounds bilateral. Which medication regimen below should be added?
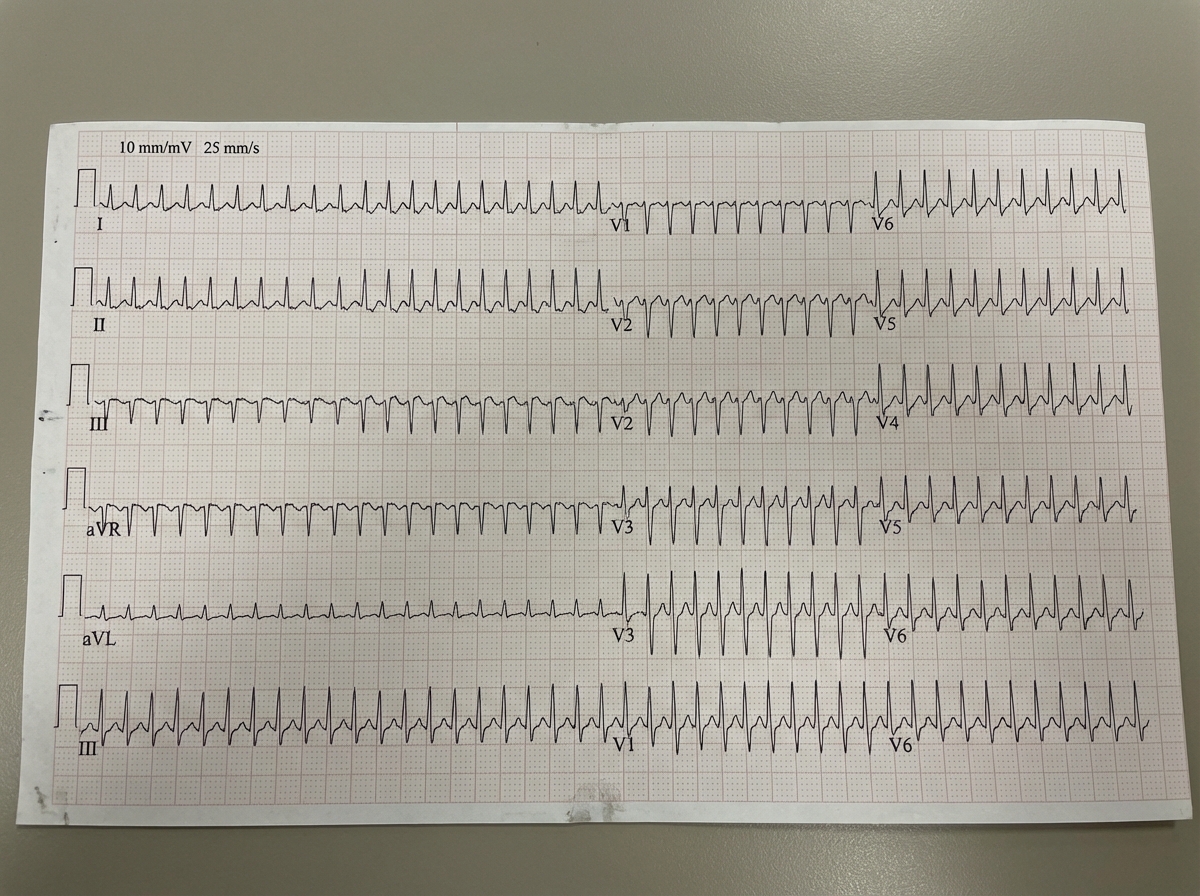
A 43-year-old man comes to the emergency room complaining of chest discomfort. He describes the feeling as "tightness," and also reports weakness and palpitations for the past hour. He denies shortness of breath, diaphoresis, or lightheadedness. He has no significant past medical history, and does not smoke, drink, or use illicit drugs. His father had a myocardial infarction at age 72. He is afebrile, heart rate is 125 bpm, and his blood pressure is 120/76. He is alert and oriented to person, place, and time. His electrocardiogram is shown below. Which of the following tests should be ordered in the initial work-up of this patient's condition?
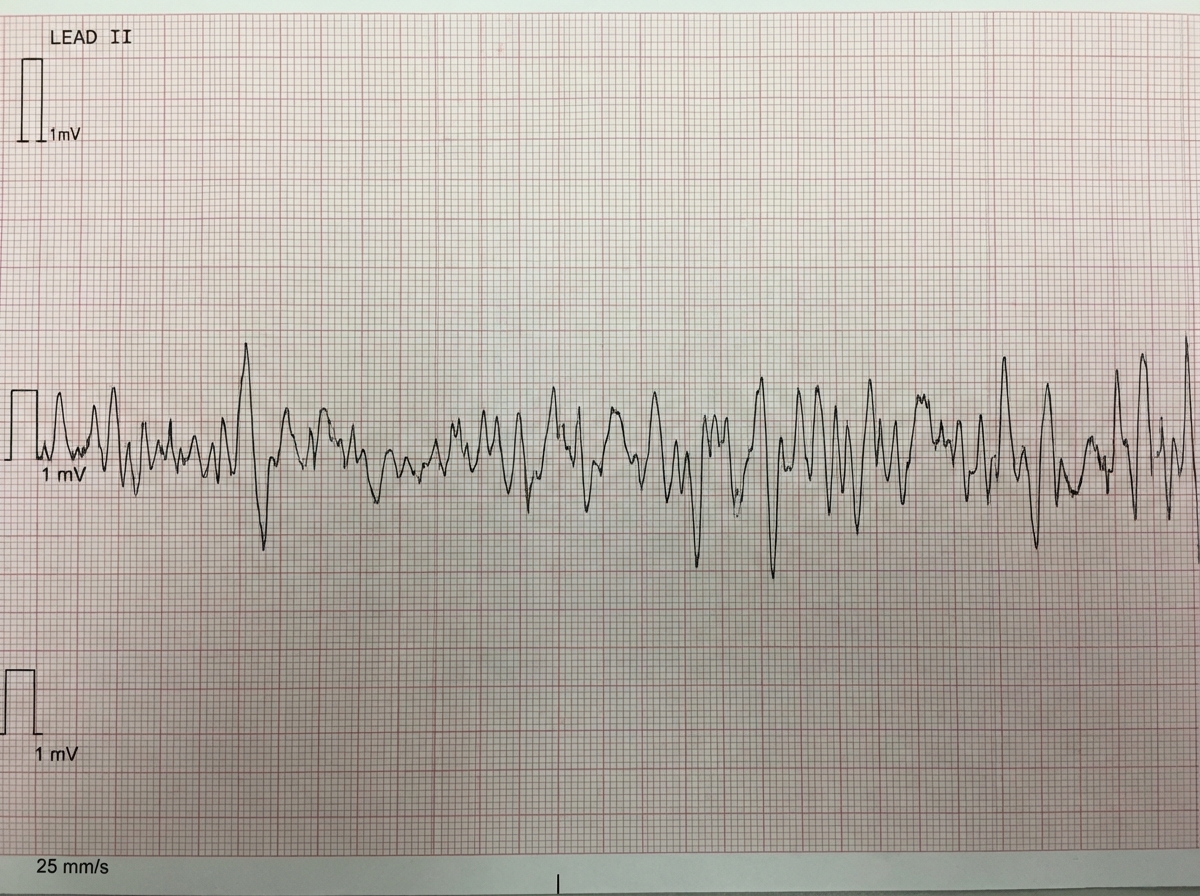
One hour after being admitted to the hospital for sharp, acute chest pain and diaphoresis, a 55-year-old woman with type 2 diabetes mellitus loses consciousness in the emergency department. There are no palpable pulses. Chest compressions are started. The patient has a history of breast cancer that was surgically treated 4 years ago. Prior to admission, the patient was on a long bus ride to visit her sister. Her medications include tamoxifen, atorvastatin, metoprolol, metformin, and insulin. Serum troponin levels are elevated. The cardiac rhythm is shown. Which of the following is the most appropriate next step in management?
Three days after undergoing cardiac catheterization and coronary angioplasty for acute myocardial infarction, a 70-year-old man develops shortness of breath at rest. He has hypertension, hyperlipidemia, and type 2 diabetes mellitus. His current medications include aspirin, clopidogrel, atorvastatin, sublingual nitroglycerin, metoprolol, and insulin. He appears diaphoretic. His temperature is 37°C (98.6°F), pulse is 120/min, respirations are 22/min, and blood pressure is 100/55 mm Hg. Crackles are heard at both lung bases. Cardiac examination shows a new grade 3/6 holosystolic murmur heard best at the cardiac apex. An ECG shows sinus rhythm with T wave inversion in leads II, III, and aVF. Which of the following is the most likely explanation for this patient's symptoms?
A 54-year-old man is brought to the emergency department 1 hour after the sudden onset of shortness of breath, epigastric pain, and sweating. He has no history of similar symptoms. He has hypertension and type 2 diabetes mellitus. Current medications include amlodipine and metformin. He has smoked one pack of cigarettes daily for 20 years. He appears weak and pale. His pulse is 56/min, respirations are 18/min, and blood pressure is 100/70 mm Hg. Cardiac examination shows elevated jugular venous pressure with normal heart sounds. The lungs are clear to auscultation. The skin is cold to the touch. A 12-lead ECG with right-sided leads is shown, demonstrating ST elevation in leads II, III, aVF, and V4R. Bedside transthoracic echocardiography shows right ventricular dysfunction with preserved left ventricular function. High-dose aspirin is administered. Administration of which of the following is most appropriate next step in management?
A 50-year-old man presents to his primary care physician with a chief complaint of chest pain that is squeezing in nature. He used to have similar symptoms in the past while playing tennis with his friends. Yesterday, while moving furniture in his new home, he experienced this pain that lasted for 20 minutes and radiated towards his jaw and shoulder. He has been diagnosed with diabetes mellitus and hypertension for over 10 years and regularly takes his medications. The pain is not associated with nausea, vomiting, food intake, sweating, or cough. On physical examination, the patient is not in acute distress. His blood pressure is 135/85 mm Hg, heart rate is 80/min, respiratory rate is 16/min, temperature is 36.9°C (98.5°F), and BMI is 30 kg/m2. On physical examination, bilateral vesicular breath sounds are heard with absent chest tenderness. Cardiovascular examination reveals normal S1 and S2 without any abnormal sounds or murmur. Abdominal examination is within normal limit. What is the most likely cause of this patient’s condition?
Seventy-two hours after admission for an acute myocardial infarction, a 48-year-old man develops dyspnea and a productive cough with frothy sputum. Physical examination shows coarse crackles in both lungs and a blowing, holosystolic murmur heard best at the apex. ECG shows Q waves in the anteroseptal leads. Pulmonary capillary wedge pressure is 23 mm Hg. Which of the following is the most likely cause of this patient’s current condition?
A 57-year-old man presents to the emergency department because of pain in the center of his chest that is radiating down his left arm and up the left side of his neck. The pain started suddenly 30 minutes ago while the patient was at work. The patient describes the pain as squeezing in nature, 10/10 in intensity, and is associated with nausea and difficulty breathing. He has had type 2 diabetes mellitus for 15 years, hypertension for 10 years, and dyslipidemia, but he denies any history of a cardiac problem. He has a 40-pack-year history of smoking but does not drink alcohol. Vital signs include: blood pressure 80/40 mm Hg, regular pulse 90/min, and temperature 37.2°C (98.9°F). Chest auscultation reveals diffuse bilateral rales with no murmurs. ECG reveals convex ST-segment elevation in leads V1 to V6 and echocardiogram shows anterolateral hypokinesis, retrograde blood flow into the left atrium, and an ejection fraction of 45%. Which of the following best describe the mechanism of this patient’s illness?
A 48-year-old man presents early in the morning to the emergency department with a burning sensation in his chest. He describes a crushing feeling below the sternum and reports some neck pain on the left side. Furthermore, he complains of difficulty breathing. Late last night, he had come home and had eaten a family size lasagna by himself while watching TV. His past medical history is significant for type 2 diabetes and poorly controlled hypertension. The patient admits he often neglects to take his medications and has not been following his advised diet. His current medications are aspirin, metformin, and captopril. Examination reveals a distressed, overweight male sweating profusely. Which of the following is most likely to be found on auscultation?
Practice by Chapter
ACS pathophysiology and classification
Practice Questions
STEMI diagnosis and management
Practice Questions
NSTEMI diagnosis and management
Practice Questions
Unstable angina
Practice Questions
Cardiac biomarkers
Practice Questions
ECG interpretation in ACS
Practice Questions
Reperfusion strategies
Practice Questions
Antiplatelet therapy
Practice Questions
Anticoagulation in ACS
Practice Questions
Complications of MI
Practice Questions
Secondary prevention
Practice Questions
Special populations (elderly, renal dysfunction)
Practice Questions
Risk stratification in ACS
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app