
ACS — MCQs

On this page
A 62-year-old man with a past medical history of previous myocardial infarction, angina, hypertension, hyperlipidemia, diabetes mellitus, peripheral vascular disease, and below knee amputation has developed new chest pain. His medication includes insulin, hydrochlorothiazide, lisinopril, metoprolol, daily aspirin, atorvastatin, and nitroglycerin as needed. His vitals include: blood pressure 135/87 mm Hg, pulse 52/min, and respirations 17/min. Coronary arteriography shows a reduced ejection fraction, a 65% stenosis of the left anterior descending artery, and a 75% stenosis of the left circumflex artery. Which of the following is the recommended treatment for the patient?
A 57-year-old man is brought to the emergency department for crushing substernal chest pain at rest for the past 2 hours. The pain began gradually while he was having an argument with his wife and is now severe. He does not take any medications. He has smoked 1 pack of cigarettes daily for 35 years. He is diaphoretic. His temperature is 37.1°C (98.8°F), pulse is 110/min, respirations are 21/min, and blood pressure is 115/65 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 97%. Cardiac examination shows an S4 gallop. The lungs are clear to auscultation. An ECG is shown. Which of the following is the most likely underlying cause of this patient's condition?
A 50-year-old man presents the emergency department for intense chest pain, profuse sweating, and shortness of breath. The onset of these symptoms was 3 hours ago. The chest pain began after a heated discussion with a colleague at the community college where he is employed. Upon arrival, he is found conscious and responsive; the vital signs include a blood pressure of 130/80 mm Hg, a heart rate at 90/min, a respiratory rate at 20/min, and a body temperature of 36.4°C (97.5°F). His medical history is significant for hypertension diagnosed 7 years ago, which is well-controlled with a calcium channel blocker. The initial electrocardiogram (ECG) shows ST-segment depression in multiple consecutive leads, an elevated cardiac troponin T level, and normal kidney function. Which of the following would you expect to find in this patient?
A 56-year-old man is brought to the Emergency Department with intense chest pain that radiates to his left arm and jaw. He also complains of feeling lightheaded. Upon arrival, his blood pressure is 104/60 mm Hg, pulse is 102/min, respiratory rate is 25/min, body temperature is 36.5°C (97.7°F), and oxygen saturation is 94% on room air. An electrocardiogram shows an ST-segment elevation in I, aVL, and V5-6. The patient is transferred to the cardiac interventional suite for a percutaneous coronary intervention. The patient is admitted to the hospital after successful revascularization. During his first night on the ICU floor his urinary output is 0.15 mL/kg/h. Urinalysis shows muddy brown casts. Which of the following outcomes specific to the patient’s condition would you expect to find?
Two days after undergoing an uncomplicated total thyroidectomy, a 63-year-old woman has acute, progressive chest pain. The pain is sharp and burning. She feels nauseated and short of breath. The patient has a history of hypertension, type 1 diabetes mellitus, medullary thyroid cancer, multiple endocrine neoplasia type 2A, anxiety, coronary artery disease, and gastroesophageal reflux disease. She smoked half a pack of cigarettes daily for 24 years but quit 18 years ago. Current medications include lisinopril, insulin glargine, insulin aspart, sertraline, aspirin, ranitidine, and levothyroxine. She appears anxious and diaphoretic. Her temperature is 37.4°C (99.3°F), pulse is 64/min, respirations are 17/min, and blood pressure is 148/77 mm Hg. The lungs are clear to auscultation. Examination shows a 3-cm linear incision over the anterior neck with 1 mm of surrounding erythema and mild serous discharge. The chest wall and abdomen are nontender. There is 5/5 strength in all extremities and decreased sensation to soft touch on the feet bilaterally. The remainder of the examination shows no abnormalities. Which of the following is the most appropriate next step in management?
A 68-year-old woman, otherwise healthy, is admitted to the coronary care unit due to acute ischemic cardiomyopathy. No other significant past medical history. Her vital signs include: pulse 116/min, respiratory rate 21/min, temperature 37.4°C (99.3°F), and blood pressure 160/100 mm Hg. On physical examination, the patient is in distress. Cardiopulmonary exam is positive for bilateral pulmonary crackles at the lung bases, tachycardia, and jugular venous distension. Her laboratory findings are significant for a hemoglobin of 7.8 g/dL. She is initially treated with oxygen, antiplatelet therapy, nitroglycerin, and beta-blockers. In spite of these treatments, her angina does not subside. The patient is not a candidate for percutaneous coronary intervention, so she is being prepared for a coronary artery bypass graft. Which of the following would be the next, best step in management of this patient?
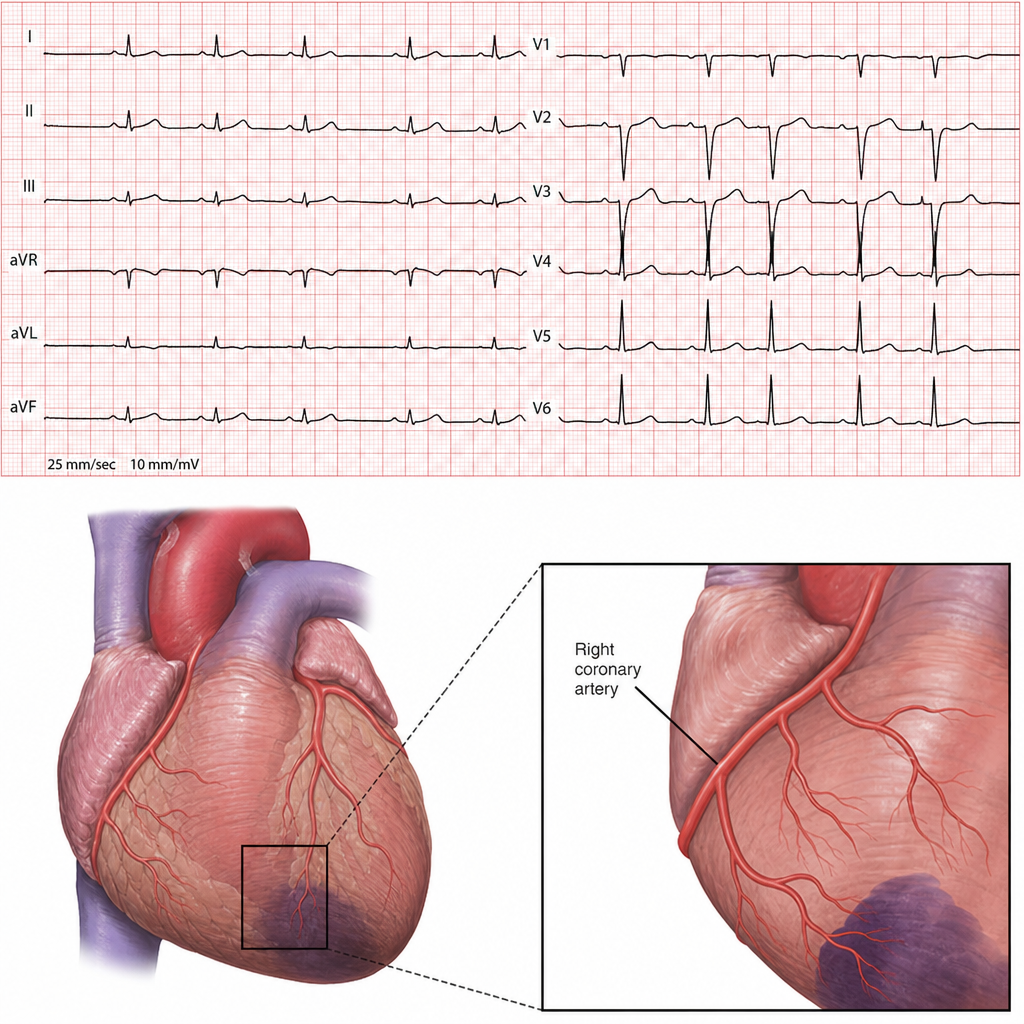
A 64-year-old male with a past medical history of obesity, diabetes, hypertension, and hyperlipidemia presents with an acute onset of nausea, vomiting, diaphoresis, and crushing substernal chest pain. Vital signs are temperature 37° C, HR 110, BP 149/87, and RR of 22 with an oxygen saturation of 99% on room air. Physical exam reveals a fourth heart sound (S4), and labs are remarkable for an elevated troponin. EKG is shown below. The pathogenesis of the condition resulting in this patient’s presentation involves:
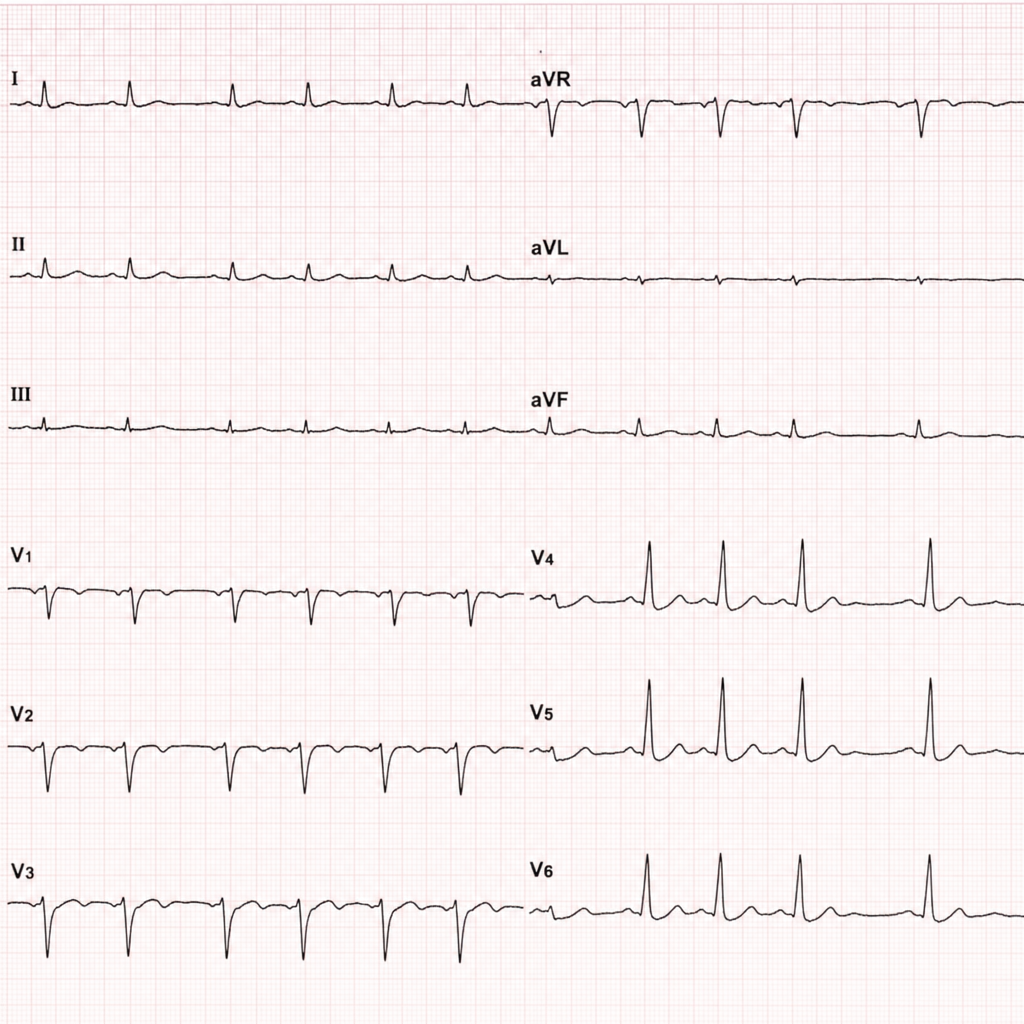
A 70-year-old man presents to the emergency department with severe substernal chest pain of one hour’s duration. The patient was taking a morning walk when the onset of pain led him to seek care. His past medical history includes coronary artery disease, hyperlipidemia, and hypertension. Medications include aspirin, losartan, and atorvastatin. An electrocardiogram reveals ST elevations in the inferior leads II, III, and avF as well as in leads V5 and V6. The ST elevations found in leads V5-V6 are most indicative of pathology in which of the following areas of the heart?
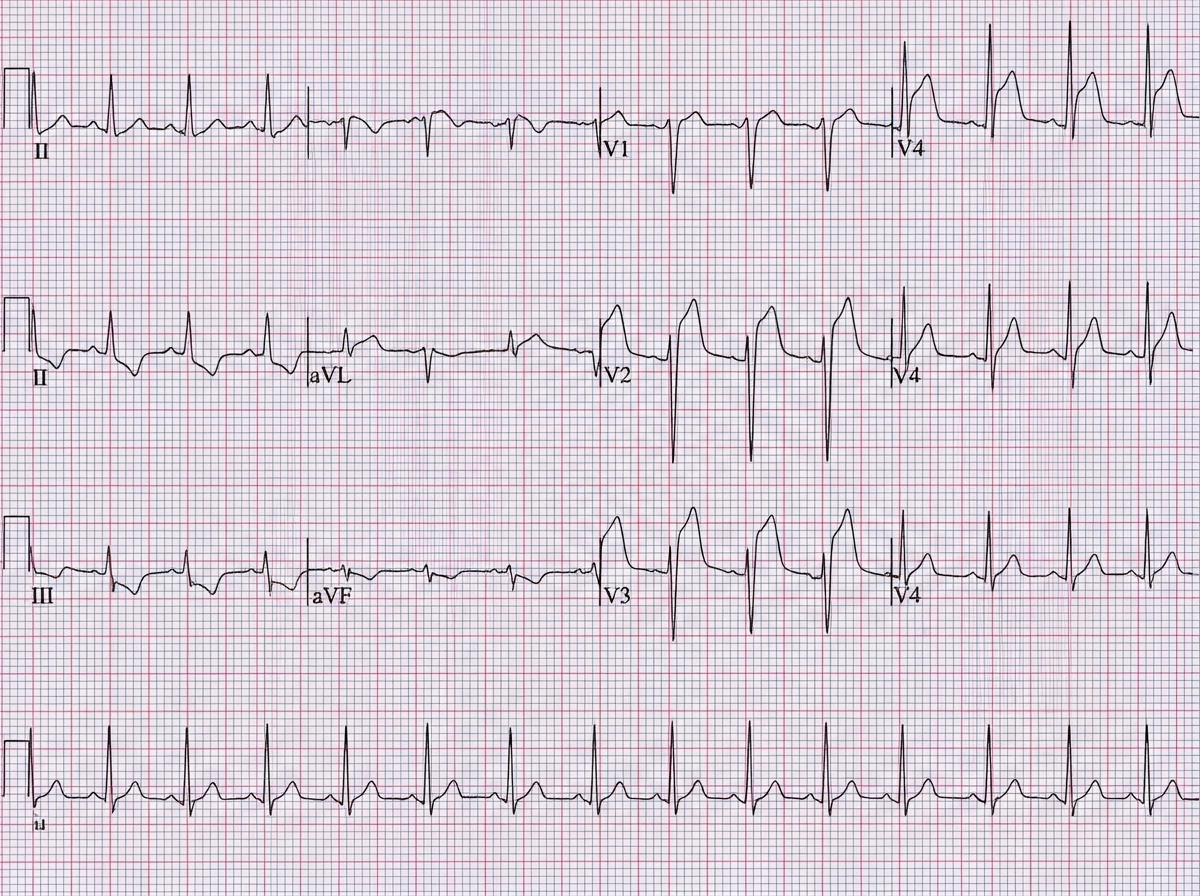
A 46-year-old man accountant is admitted to the emergency department with complaints of retrosternal crushing pain that radiates to his left arm and jaw. The medical history is significant for hyperlipidemia and arterial hypertension, for which he is prescribed a statin and ACE inhibitor, respectively. An ECG is obtained and shows an ST-segment elevation in leads avF and V2-V4. The blood pressure is 100/50 mm Hg, the pulse is 120/min, and the respiratory rate is 20/min. His BMI is 33 kg/m2 and he has a 20-year history of smoking cigarettes. Troponin I is elevated. The patient undergoes percutaneous coronary intervention immediately after admission. Angioplasty and stenting were successfully performed. On follow-up the next day, the ECG shows decreased left ventricular function and local hypokinesia. The patient is re-evaluated 14 days later. The echocardiography reveals a normal ejection fraction and no hypokinesis. Which of the phenomena below explains the patient’s clinical course?
A 49-year-old woman is brought in to the emergency department by ambulance after developing crushing chest pain and palpitations. Past medical history is significant for hypertension, hyperlipidemia, and obesity. She takes chlorthalidone, lisinopril, atorvastatin, metformin, and an oral contraceptive every day. She works as a lawyer and her job is stressful. She drinks wine with dinner every night and smokes 10 cigarettes a day. Emergency personnel stabilized her and administered oxygen while on the way to the hospital. Upon arrival, the vital signs include: blood pressure 120/80 mm Hg, heart rate 120/min, respiratory rate 22/min, and temperature 37.7°C (99.9°F). On physical exam, she is an obese woman in acute distress. She is diaphoretic and has difficulty catching her breath. A bedside electrocardiogram (ECG) is performed which reveals ST-segment elevation in leads II, III, and aVF. Which of the following is the most probable diagnosis?
Practice by Chapter
ACS pathophysiology and classification
Practice Questions
STEMI diagnosis and management
Practice Questions
NSTEMI diagnosis and management
Practice Questions
Unstable angina
Practice Questions
Cardiac biomarkers
Practice Questions
ECG interpretation in ACS
Practice Questions
Reperfusion strategies
Practice Questions
Antiplatelet therapy
Practice Questions
Anticoagulation in ACS
Practice Questions
Complications of MI
Practice Questions
Secondary prevention
Practice Questions
Special populations (elderly, renal dysfunction)
Practice Questions
Risk stratification in ACS
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app