
ACS — MCQs

On this page
Two days after coronary artery stent placement for a posterior myocardial infarction, a 70-year-old woman complains of difficulty breathing and retrosternal chest pain. She has a history of atrial fibrillation, for which she takes verapamil. Following stent placement, the patient was started on aspirin and clopidogrel. She appears to be in acute distress and is disoriented. Respirations are 22/min. Pulse oximetry on room air shows an oxygen saturation of 80%. Diffuse crackles are heard on auscultation of the chest. The patient is intubated and mechanical ventilation is started. Shortly afterwards, she becomes unresponsive. Heart sounds are inaudible and her carotid pulses are not palpable. The cardiac monitor shows normal sinus rhythm with T-wave inversion. Which of the following is the most appropriate next step in management?
A 57-year-old man presents to his primary care provider because of chest pain for the past 3 weeks. The chest pain occurs after climbing more than 2 flights of stairs or walking for more than 10 minutes. His symptoms remain for an average of 30 minutes despite rest, but they eventually remit. He is obese, has a history of type 2 diabetes mellitus, and has smoked 15–20 cigarettes a day for the past 25 years. His father died from a myocardial infarction at 52 years of age. His vital signs reveal a temperature of 36.7°C (98.0°F), blood pressure of 145/93 mm Hg, and a heart rate of 85/min. The physical examination is unremarkable. Which of the following is consistent with unstable angina?
A 60-year-old man with a history of hypertension, diabetes, and hyperlipidemia was successfully managed for acute myocardial infarction involving the left anterior descending artery. Eight months after his discharge home, an echocardiogram reveals the presence of a ventricular aneurysm. The patient subsequently dies after a stroke. Which of the following best explains the sequence of events leading to this outcome?
A 58-year-old man comes to the emergency department for complaints of crushing chest pain for 4 hours. He was shoveling snow outside when the pain started. It is rated 7/10 and radiates to his left arm. An electrocardiogram (ECG) demonstrates ST-segment elevation in leads V2-4. He subsequently undergoes percutaneous coronary intervention (PCI) and is discharged with aspirin, clopidogrel, carvedilol, atorvastatin, and lisinopril. Five days later, the patient is brought to the emergency department by his wife with complaints of dizziness. He reports lightheadedness and palpitations for the past 2 hours but otherwise feels fine. His temperature is 99.7°F (37.6°C), blood pressure is 95/55 mmHg, pulse is 105/min, and respirations are 17/min. A pulmonary artery catheter is performed and demonstrates an increase in oxygen concentration at the pulmonary artery. What finding would you expect in this patient?
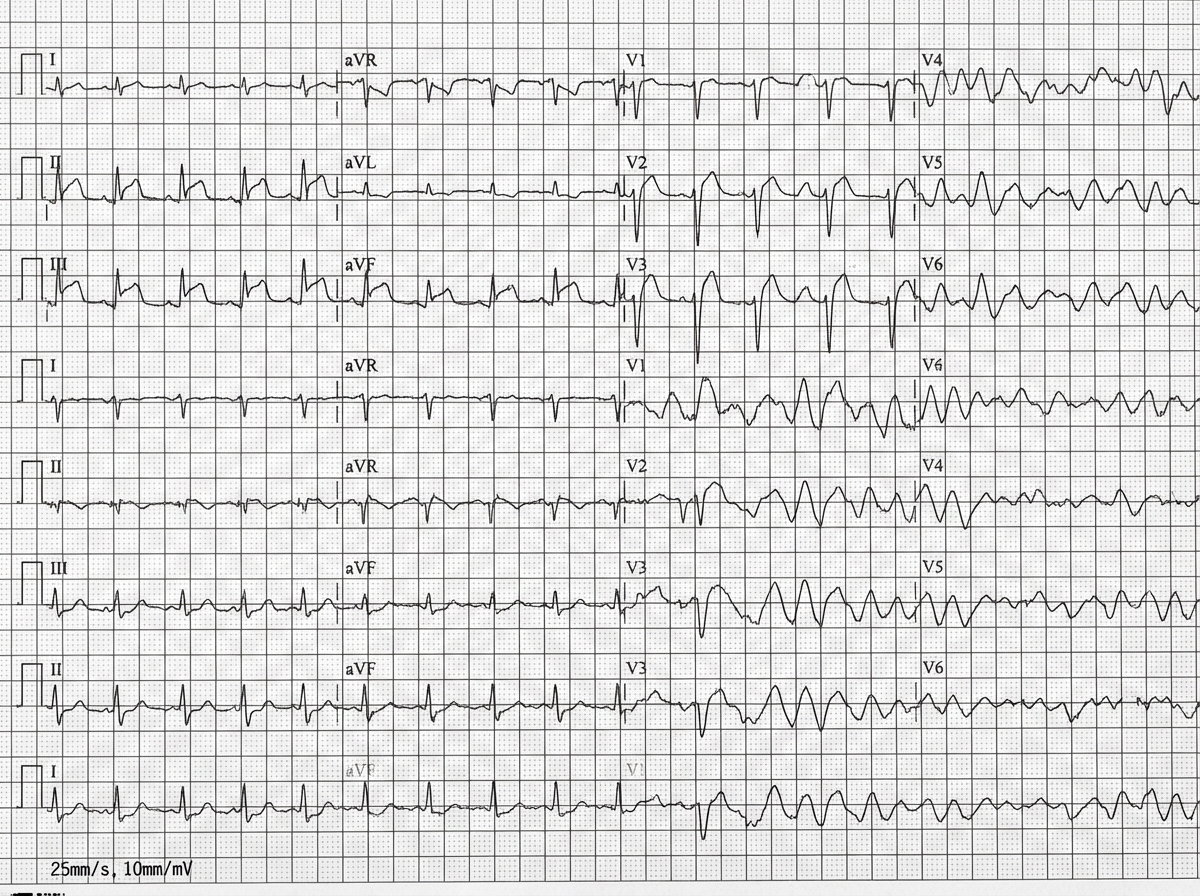
A 42-year-old man is brought to the emergency department 20 minutes after the sudden onset of severe chest pain, diaphoresis, shortness of breath, and palpitations. His symptoms occurred while he was at a party with friends. He has smoked one pack of cigarettes daily for 24 years. He uses cocaine occasionally. The last use was three hours ago. He appears pale. His pulse is 110/min, blood pressure is 178/106 mm Hg, and respirations are 24/min. His pupils are dilated and react sluggishly to light. The lungs are clear to auscultation. An ECG shows tachycardia and ST segment elevation in leads II, III, and aVF. While recording the ECG, the patient loses consciousness. A photo of the ECG at that point is shown. Which of the following is the most appropriate next step in management?
A 67-year-old man presents to the emergency department for squeezing and substernal chest pain. He states that he was at home eating dinner when his symptoms began. The patient has a past medical history of diabetes, hypertension, and dyslipidemia. He is currently taking atorvastatin, lisinopril, insulin, metformin, metoprolol, and aspirin. Six days ago he underwent percutaneous coronary intervention. His temperature is 99.5°F (37.5°C), blood pressure is 197/118 mmHg, pulse is 120/min, respirations are 17/min, and oxygen saturation is 98% on room air. Physical exam reveals an uncomfortable elderly man who is sweating. An ECG is ordered. Which of the following is the best next step in management for this patient?
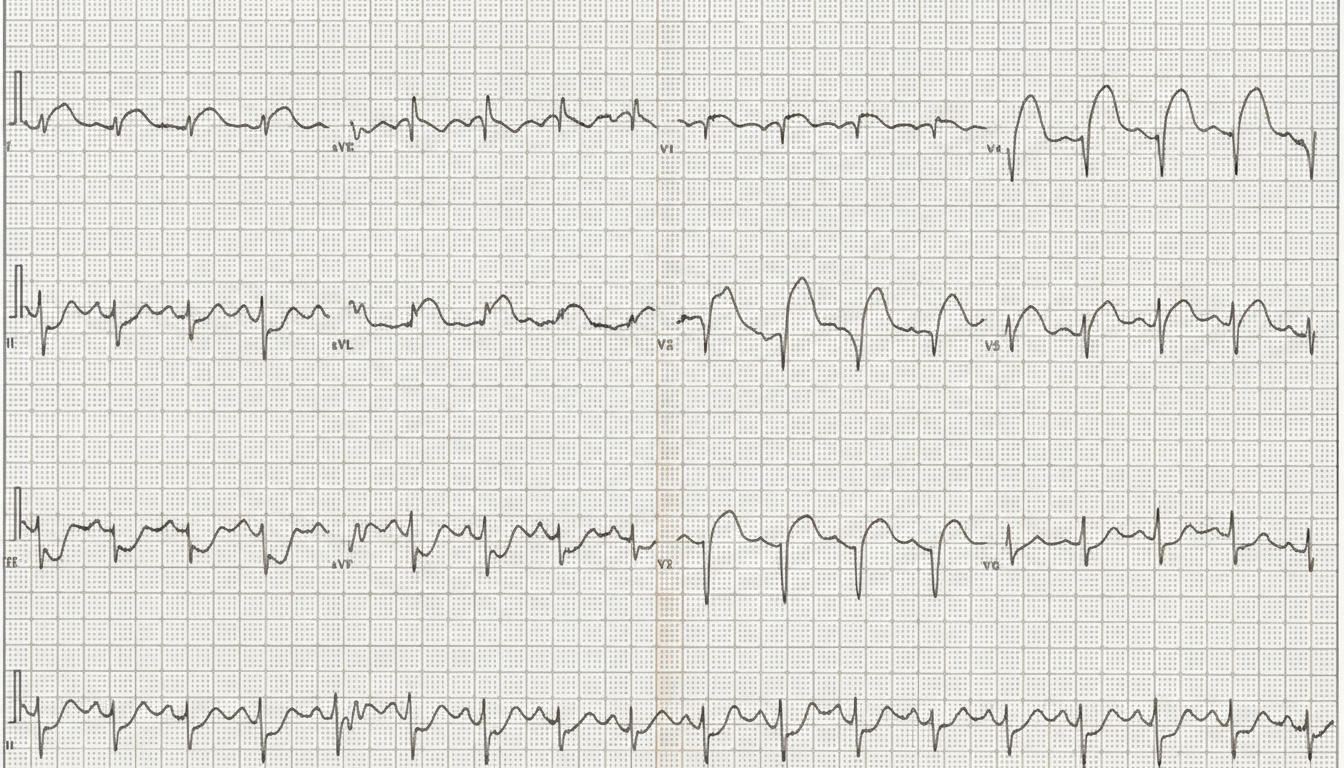
A 64-year-old man presents to the emergency department with sudden onset of chest pain and an episode of vomiting. He also complains of ongoing nausea and heavy sweating (diaphoresis). He denies having experienced such symptoms before and is quite upset. Medical history is significant for hypertension and types 2 diabetes mellitus. He currently smokes and has smoked at least half a pack daily for the last 40 years. Vitals show a blood pressure of 80/50 mm Hg, pulse of 50/min, respirations of 20/min, temperature of 37.2°C (98.9°F), and oximetry is 99% before oxygen by facemask. Except for the patient being visibly distressed and diaphoretic, the examination is unremarkable. ECG findings are shown in the picture. Where is the most likely obstruction in this patient’s cardiac blood supply?
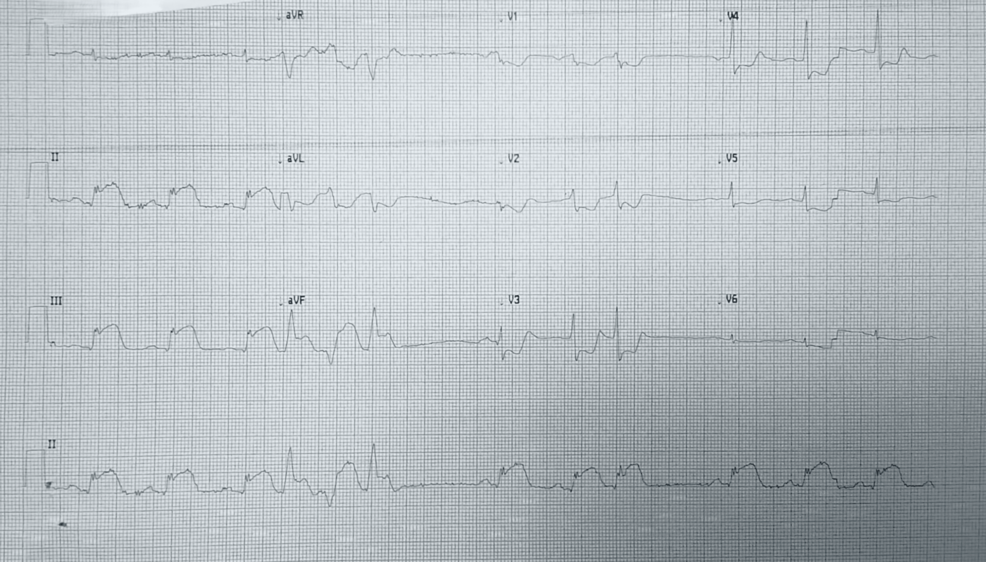
A 57-year-old man with a known angina pectoris starts to experience a severe burning retrosternal pain that radiates to his left hand. After 2 consecutive doses of sublingual nitroglycerin taken 5 minutes apart, there is no improvement in his symptoms, and the patient calls an ambulance. Emergency medical service arrives within 10 minutes and begins evaluation and prehospital management. The vital signs include: blood pressure 85/50 mm Hg, heart rate 96/min, respiratory rate 19/min, temperature 37.1℃ (98.9℉), and SpO2 89% on ambient air. Oxygen supply and intravenous access are established. An ECG shows the findings in the given image. Which of the following is a part of a proper further prehospital management strategy for this patient?
A 66-year-old man comes to the emergency department because of a 1-day history of chest pain, palpitations, and dyspnea on exertion. He had a similar episode 3 days ago and was diagnosed with an inferior wall myocardial infarction. He was admitted and a percutaneous transluminal coronary angioplasty was successfully done that day. A fractional flow reserve test during the procedure showed complete resolution of the stenosis. Laboratory tests including serum glucose, lipids, and blood count were within normal limits. He was discharged the day after the procedure on a drug regimen of aspirin, simvastatin, and isosorbide dinitrate. At the time of discharge, he had no chest pain or dyspnea. Presently, his vitals are normal and ECG at rest shows new T-wave inversion. Which of the following is the most reliable test for rapidly establishing the diagnosis in this patient?
A 65-year-old man presents to the emergency department for sudden weakness. He was doing mechanical work on his car where he acutely developed right-leg weakness and fell to the ground. He is accompanied by his wife, who said that this has never happened before. He was last seen neurologically normal approximately 2 hours prior to presentation. His past medical history is significant for hypertension and type II diabetes. His temperature is 98.8°F (37.1°C), blood pressure is 177/108 mmHg, pulse is 90/min, respirations are 15/min, and oxygen saturation is 99% on room air. Neurological exam reveals that he is having trouble speaking and has profound weakness of his right upper and lower extremity. Which of the following is the best next step in management?
Practice by Chapter
ACS pathophysiology and classification
Practice Questions
STEMI diagnosis and management
Practice Questions
NSTEMI diagnosis and management
Practice Questions
Unstable angina
Practice Questions
Cardiac biomarkers
Practice Questions
ECG interpretation in ACS
Practice Questions
Reperfusion strategies
Practice Questions
Antiplatelet therapy
Practice Questions
Anticoagulation in ACS
Practice Questions
Complications of MI
Practice Questions
Secondary prevention
Practice Questions
Special populations (elderly, renal dysfunction)
Practice Questions
Risk stratification in ACS
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app