
Complications of MI — MCQs

A 28-year-old male presents with sharp, stabbing chest pain that worsens when lying flat and improves when sitting forward. He reports a recent viral upper respiratory infection 2 weeks ago. On examination, a friction rub is heard on auscultation. His vital signs are stable. An ECG is most likely to show which of the following findings in this patient?
A 55-year-old man with a past medical history of obesity and hyperlipidemia suddenly develops left-sided chest pain and shortness of breath while at work. He relays to coworkers that the pain is intense and has spread to his upper left arm over the past 10 minutes. He reports it feels a lot like the “heart attack” he had a year ago. He suddenly collapses and is unresponsive. Coworkers perform cardiopulmonary resuscitation for 18 minutes until emergency medical services arrives. Paramedics pronounce him dead at the scene. Which of the following is the most likely cause of death in this man?
A 53-year-old man with a past medical history significant for hyperlipidemia, hypertension, and hyperhomocysteinemia presents to the emergency department complaining of 10/10 crushing, left-sided chest pain radiating down his left arm and up his neck into the left side of his jaw. His ECG shows ST-segment elevation in leads V2-V4. He is taken to the cardiac catheterization laboratory for successful balloon angioplasty and stenting of a complete blockage in his left anterior descending coronary artery. Echocardiogram the following day shows decreased left ventricular function and regional wall motion abnormalities. A follow-up echocardiogram 14 days later shows a normal ejection fraction and no regional wall motion abnormalities. This post-infarct course illustrates which of the following concepts?
A 73-year-old man presents to the emergency department with acute substernal chest pain that began a few hours ago. The pain is described as a "pressure" that radiates to his left arm. His past medical history is significant for hypertension and hyperlipidemia. He is on chlorthalidone for his hypertension and simvastatin for hyperlipidemia. He has a 30 pack-year history of smoking and drinks 1-2 beers on weekends. His EKG shows ST depressions in the anterior precordial leads and he is given the proper medications and sent for emergency revascularization. Seven days later, he develops dyspnea that worsens in the supine position. Bibasilar crackles are heard on pulmonary auscultation. Cardiac exam reveals a new 3/6 holosystolic murmur best heard at the apex with radiation to the axilla. What is the most likely etiology of this patient's new symptoms?
A 40-year-old Caucasian male presents to the emergency room after being shot in the arm in a hunting accident. His shirt is soaked through with blood. He has a blood pressure of 65/40, a heart rate of 122, and his skin is pale, cool to the touch, and moist. This patient is most likely experiencing all of the following EXCEPT:
A 72-year-old man presents to the emergency department because of difficulty breathing and sharp chest pain. The chest pain increases in intensity with lying down, and it radiates to the scapular ridge. Approximately 3 weeks ago, he had an anterior ST-elevation myocardial infarction, which was treated with intravenous alteplase. He was discharged home in a stable condition. Current vital signs include a temperature of 38.1 (100.5°F), blood pressure of 131/91 mm Hg, and pulse of 99/min. On examination, heart sounds are distant and a scratching sound is heard on the left sternal border. ECG reveals widespread concave ST elevations in the precordial leads and PR depressions in leads V2-V6. Which of the following is the most likely cause of this patient condition?
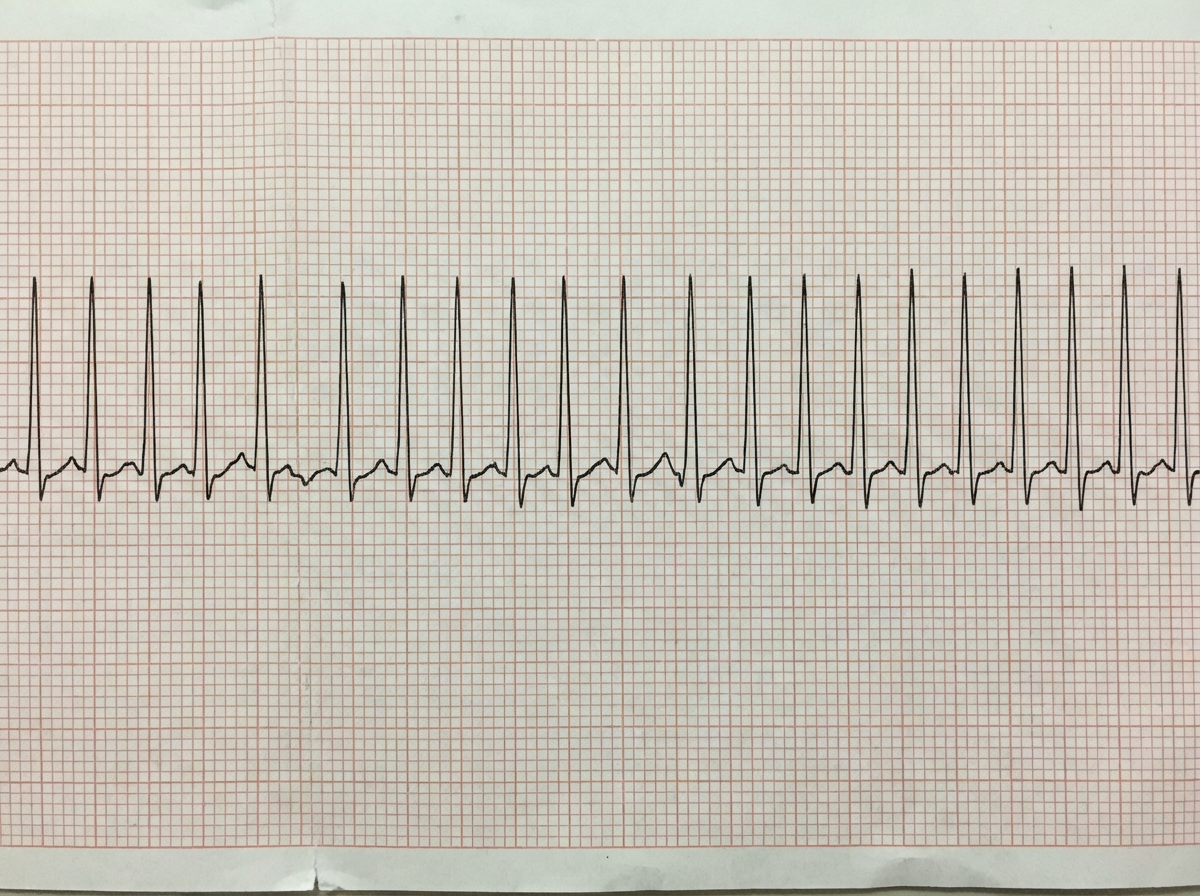
A previously healthy 33-year-old woman comes to the emergency department because she could feel her heart racing intermittently for the last 2 hours. Each episode lasts about 10 minutes. She does not have any chest pain. Her mother died of a heart attack and her father had an angioplasty 3 years ago. She has smoked a half pack of cigarettes daily for 14 years. She drinks one to two beers daily. She appears anxious. Her temperature is 37.6°C (98.1°F), pulse is 160/min, and blood pressure is 104/76 mm Hg. The lungs are clear to auscultation. Cardiac examination shows no murmurs, rubs, or gallops. An ECG is shown. Which of the following is the most appropriate initial step in management?
Two days after being admitted for acute myocardial infarction, a 61-year-old man has sharp, substernal chest pain that worsens with inspiration and improves when leaning forward. Cardiac examination shows a scratchy sound best heard over the left sternal border. Histopathological examination of the infarcted myocardial tissue is most likely to show which of the following findings?
An 80-year-old man presents to the emergency department because of gnawing substernal chest pain that started an hour ago and radiates to his neck and left jaw. A 12-lead ECG is obtained and shows ST-segment elevation with newly developing Q waves. He is admitted for treatment. 4 days after hospitalization he suddenly develops altered mental status, and his blood pressure falls from 115/75 mm Hg to 80/40 mm Hg. Physical examination shows jugular venous distention, pulsus paradoxus, and distant heart sounds. What is the most likely cause of this patient's condition?
Four days after being admitted to the intensive care unit for acute substernal chest pain and dyspnea, an 80-year-old man is evaluated for hypotension. Coronary angiography on admission showed an occlusion in the left anterior descending artery, and a drug-eluting stent was placed successfully. The patient has a history of hypertension and type 2 diabetes mellitus. Current medications include aspirin, clopidogrel, metoprolol, lisinopril, and atorvastatin. His temperature is 37.2 °C (99 °F), pulse is 112/min, respirations are 21/min, and blood pressure is 72/50 mm Hg. Cardiac examination shows a normal S1 and S2 and a new harsh, holosystolic murmur heard best at the left sternal border. There is jugular venous distention and a right parasternal heave. The lungs are clear to auscultation. Pitting edema extends up to the knees bilaterally. An ECG shows Q waves in the inferior leads. Which of the following is the most likely cause of this patient’s hypotension?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app