
ACS — MCQs

On this page
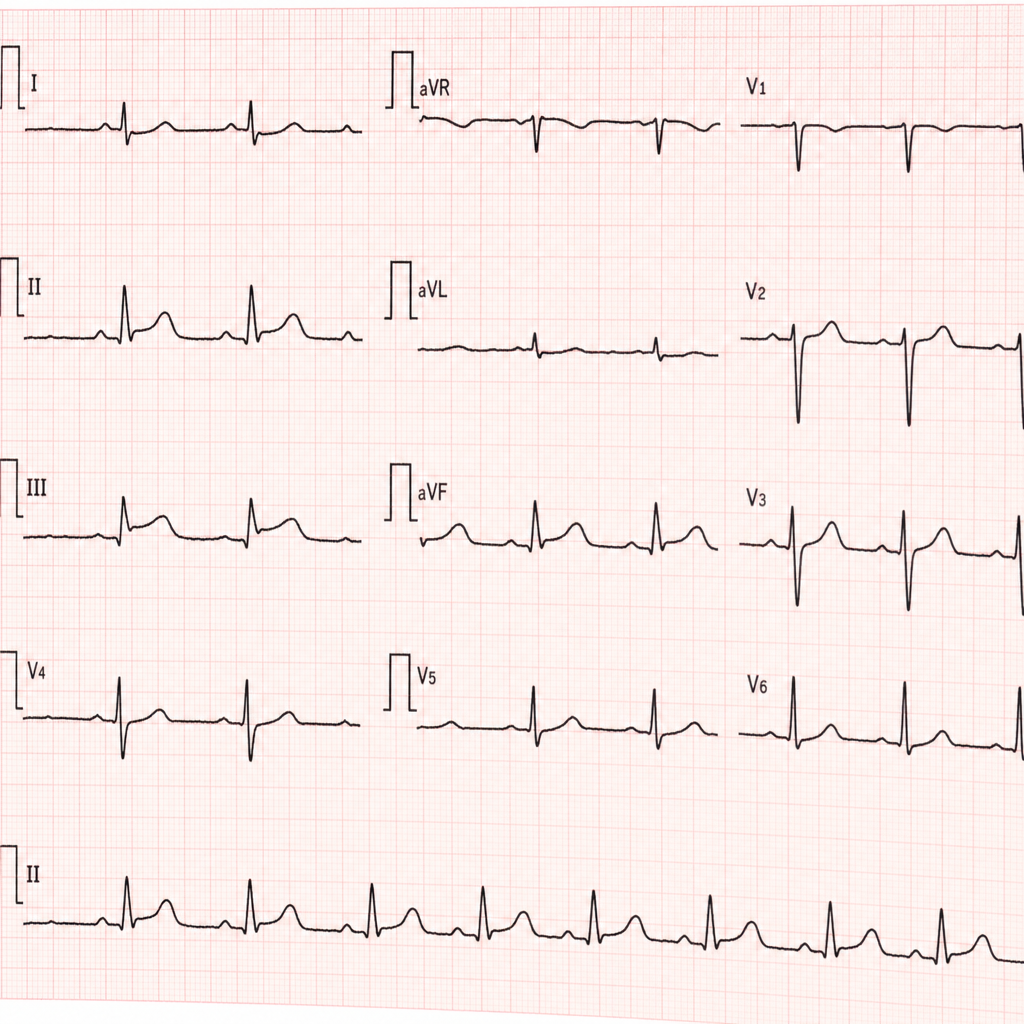
A 67-year-old woman with a history of hypertension and type 2 diabetes presents to the emergency department with 3 hours of epigastric discomfort, nausea, and diaphoresis. She denies chest pain or shortness of breath. Her blood pressure is 148/92 mmHg, heart rate is 98 bpm, and oxygen saturation is 96% on room air. Physical examination is unremarkable. An ECG is obtained and shown above. The ECG demonstrates ST-segment elevations of 2–3 mm in leads II, III, and aVF, with reciprocal ST-segment depressions in leads I and aVL, and no ST changes in the precordial leads. Which of the following is the most appropriate immediate next step in management?
Practice by Chapter
ACS pathophysiology and classification
Practice Questions
STEMI diagnosis and management
Practice Questions
NSTEMI diagnosis and management
Practice Questions
Unstable angina
Practice Questions
Cardiac biomarkers
Practice Questions
ECG interpretation in ACS
Practice Questions
Reperfusion strategies
Practice Questions
Antiplatelet therapy
Practice Questions
Anticoagulation in ACS
Practice Questions
Complications of MI
Practice Questions
Secondary prevention
Practice Questions
Special populations (elderly, renal dysfunction)
Practice Questions
Risk stratification in ACS
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app