
Screening guidelines — MCQs

On this page
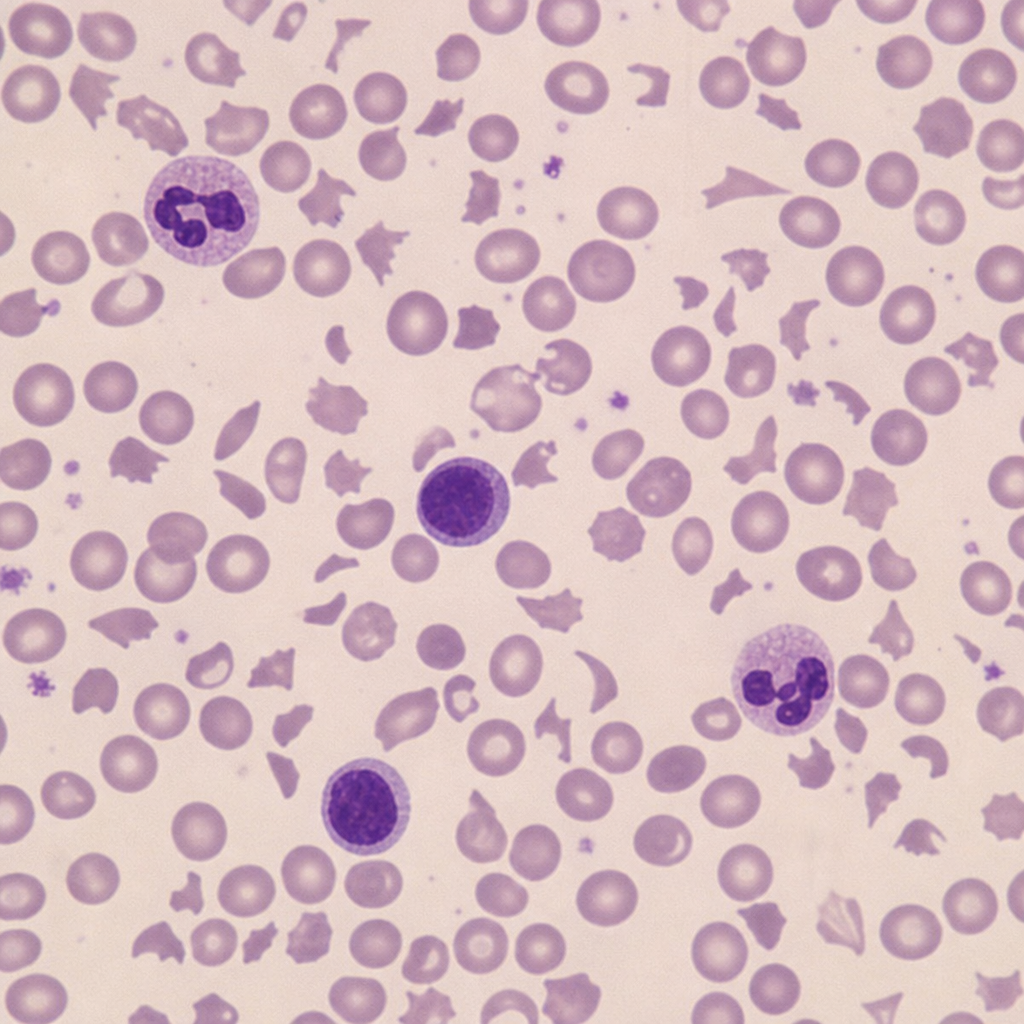
A peripheral blood smear from a 45-year-old woman with a 2-week history of fatigue, jaundice, and confusion is shown. She was recently started on ticlopidine following coronary stent placement. Her laboratory values include: hemoglobin 7.1 g/dL, platelets 18,000/µL, creatinine 2.8 mg/dL, LDH 980 U/L, and indirect bilirubin 3.4 mg/dL. Direct Coombs test is negative. The image demonstrates the most diagnostically discriminating finding. Based on the peripheral smear finding and the complete clinical picture, what is the most likely diagnosis?
A 67-year-old man with a history of hypertension and hyperlipidemia presents to the emergency department with sudden-onset tearing chest pain radiating to the back, beginning 45 minutes ago. Blood pressure is 185/100 mmHg in the right arm and 155/85 mmHg in the left arm. Heart rate is 102 bpm. He is diaphoretic and hemodynamically stable. ECG shows sinus tachycardia with no ST changes. Troponin I is pending. Chest radiograph is shown. Which of the following is the most appropriate next diagnostic step?

A 28-year-old asymptomatic pregnant woman at 12 weeks gestation presents for prenatal care. She has no personal or family history of diabetes. Her BMI is 32 kg/m². She had a random glucose of 118 mg/dL at her first visit. She asks about gestational diabetes screening. Considering her risk factors and current pregnancy, what is the most appropriate screening approach?
A 66-year-old man underwent screening colonoscopy which revealed a 1.2 cm tubular adenoma with low-grade dysplasia in the sigmoid colon that was completely removed. He has no family history of colorectal cancer. His colonoscopy 8 years ago was normal. He asks about surveillance recommendations. Considering current guidelines and competing risks, what is the most appropriate surveillance interval?
A 32-year-old woman presents for preconception counseling. She is healthy with no medical problems. Her mother and maternal aunt both had breast cancer diagnosed at ages 38 and 42, respectively. Her maternal grandmother died of ovarian cancer at age 52. The patient tested negative for BRCA1 and BRCA2 mutations 2 years ago through a commercial genetic testing panel. She asks about breast cancer screening recommendations. What is the most appropriate evaluation and management?
A 45-year-old woman presents requesting colorectal cancer screening after her sister was recently diagnosed with colon cancer at age 48. Further history reveals her sister's cancer was found to have microsatellite instability-high (MSI-H) features. The patient has no personal history of polyps or cancer and no gastrointestinal symptoms. Her sister is undergoing genetic testing for Lynch syndrome. What is the most appropriate next step in screening for this patient?
A 72-year-old woman with well-controlled hypertension and hyperlipidemia presents for follow-up. She has been getting annual mammograms since age 40. Her most recent mammogram 10 months ago was normal. She has no family history of breast cancer and has never had an abnormal mammogram. She asks if she should continue screening. Her life expectancy is estimated at 12 years based on comorbidity indices. What is the most appropriate recommendation?
A 62-year-old man with type 2 diabetes presents with a positive fecal immunochemical test (FIT) during routine screening. He has no gastrointestinal symptoms, family history of colorectal cancer, or prior colonoscopy. His hemoglobin is 13.2 g/dL. He had a screening colonoscopy 4 years ago that showed only small hyperplastic polyps. He asks if he needs another colonoscopy. What is the best approach?
A 25-year-old sexually active woman presents for her annual examination. She has had 2 lifetime sexual partners and is currently in a monogamous relationship. Her last Pap smear was at age 21 and was normal. She has no history of abnormal Pap smears or STIs. What is the most appropriate cervical cancer screening recommendation?
A 58-year-old African American man presents for a health maintenance visit. His father was diagnosed with prostate cancer at age 72. The patient asks about prostate cancer screening. His physical examination and review of systems are unremarkable. What is the most appropriate approach to prostate cancer screening for this patient?
Practice by Chapter
Principles of screening
Practice Questions
Cancer screening recommendations (by cancer type)
Practice Questions
Cardiovascular disease screening
Practice Questions
Infectious disease screening
Practice Questions
Mental health screening
Practice Questions
Developmental screening in pediatrics
Practice Questions
Geriatric screening protocols
Practice Questions
Prenatal screening
Practice Questions
Evidence basis for screening recommendations
Practice Questions
Risk-stratified screening approaches
Practice Questions
Special population screening considerations
Practice Questions
Screening interval determination
Practice Questions
Limitations and controversies in screening
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app