
Histology — MCQs

On this page
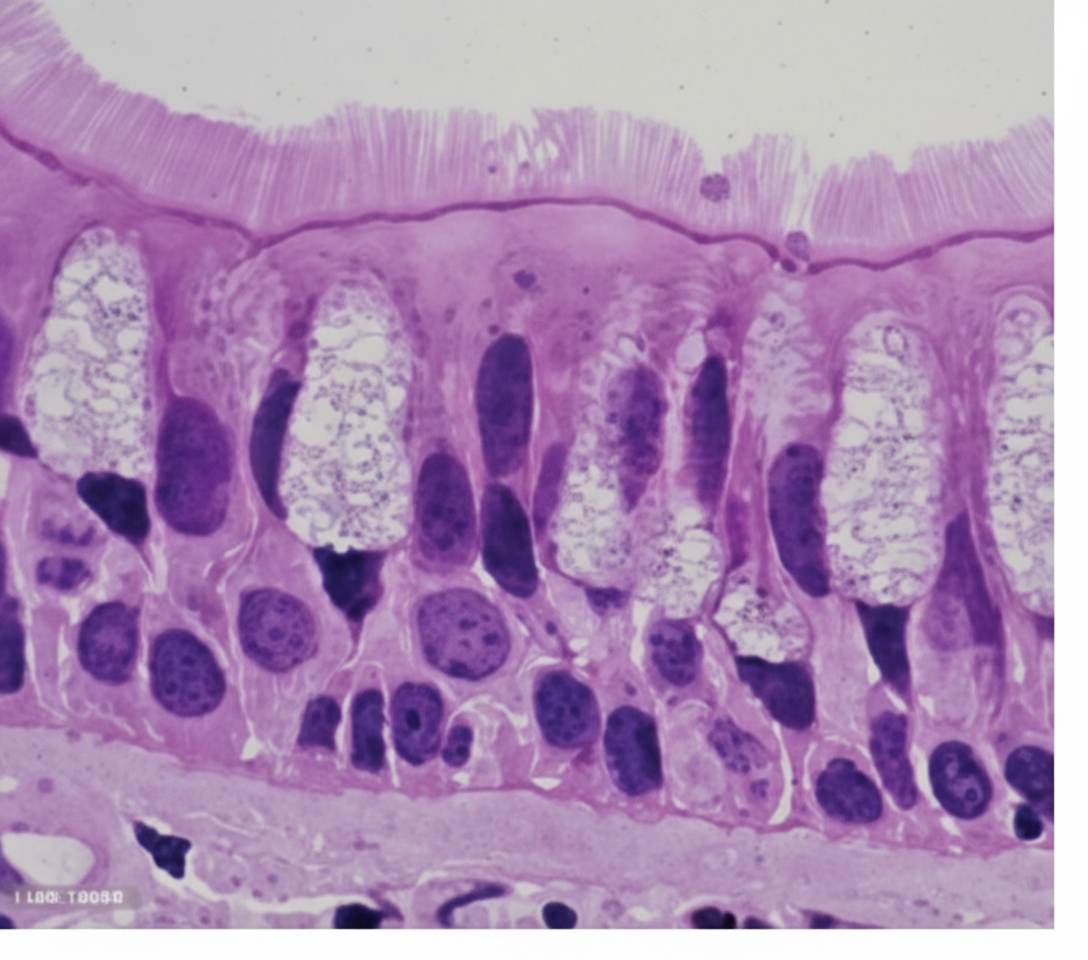
This type of epithelium is most commonly seen in which of the following organs?
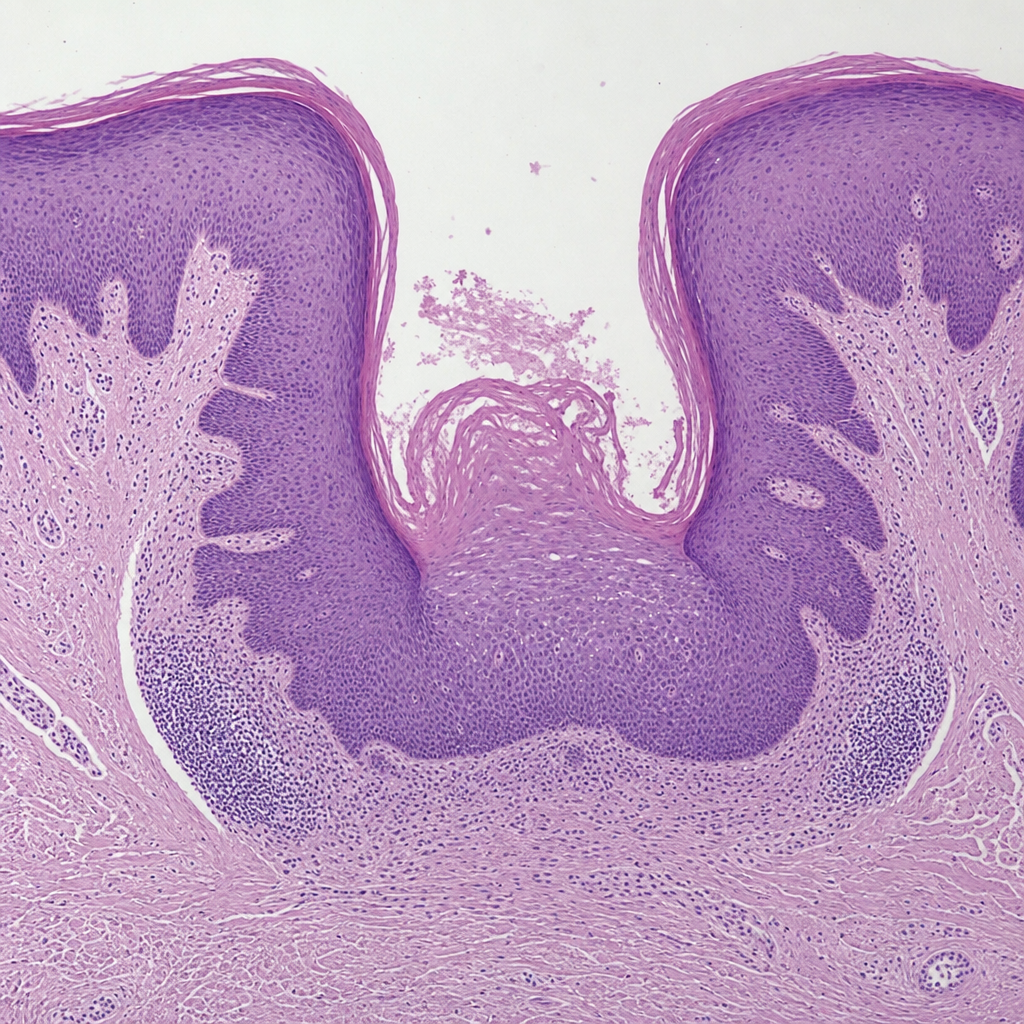
Identify the type of papillae of the tongue shown in the histological image below:
An investigator is conducting a study to document the histological changes in the respiratory tree of a chronic smoker. He obtains multiple biopsy samples from the respiratory system of a previously healthy 28-year-old man. Histopathological examination of one sample shows simple cuboidal cells with a surrounding layer of smooth muscle. Chondrocytes and goblet cells are absent. This specimen was most likely obtained from which of the following parts of the respiratory system?
A 38-year-old man comes to the physician because of a 6-month history of chest discomfort and progressive dyspnea. He cannot do daily chores without feeling out of breath. He was diagnosed in childhood with a milder X-linked dystrophinopathy that has caused progressive proximal muscle weakness and gait abnormalities over the years. Physical examination shows a waddling gait and weak patellar reflexes. Cardiovascular examination shows a holosystolic murmur, displaced point of maximal impulse, and bilateral pitting edema of the ankles. Laboratory studies show elevated levels of brain natriuretic peptide. Which of the following is the most likely underlying cause of this patient's muscle weakness?
An investigator is examining tissue samples from various muscle tissue throughout the body. She notices that biopsies collected from a specific site have a high concentration of sarcoplasmic reticulum, mitochondria, and myoglobin; they also stain poorly for ATPase. Additionally, the cell surface membranes of the myocytes in the specimen lack voltage-gated calcium channels. These myocytes are found in the greatest concentration at which of the following sites?
A 24-year-old male with cystic fibrosis is brought to the emergency room by his mother after he had difficulty breathing. He previously received a lung transplant 6 months ago and was able to recover quickly from the operation. He is compliant with all of his medications and had been doing well with no major complaints until 2 weeks ago when he began to experience shortness of breath. Exam reveals a decreased FEV1/FVC ratio and biopsy reveals lymphocytic infiltration. Which of the following components is present in the airway zone characteristically affected by the most likely cause of this patient's symptoms?
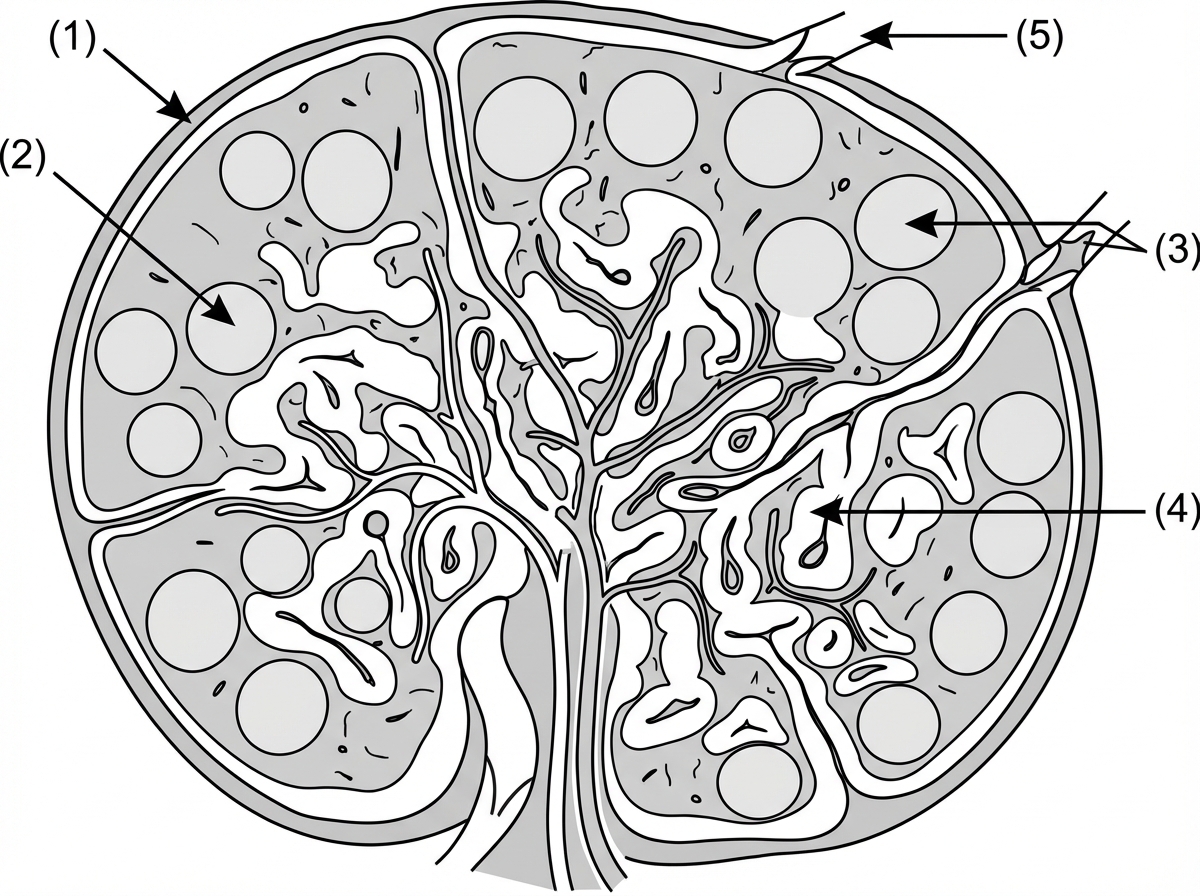
A 3-year-old boy goes camping with his parents in the Appalachian mountains of Western North Carolina. While on the hiking trip, he is exposed to an antigen. After the exposure, this antigen is phagocytosed by an antigen-presenting cell and is presented on an MHC class II molecule to a CD4+ T helper cell. This CD4+ T helper cell then encounters a B cell in the lymph node shown in the image below. The mature B cell proliferates and differentiates to produce antibodies to target this antigen. In which of the following numbered sections of the lymph node does this B cell differentiation and proliferation most likely occur?
An 82-year-old woman presents to the emergency department after a fall. Imaging reveals diffuse trauma to the left humerus from the midshaft to the distal metaphysis with shearing of the periosteum. The orthopedic surgeon suggests a follow-up in 2 weeks. In that time, the patient develops worsening pain. At follow-up, she is found to have diffuse bone necrosis from the midshaft of the left humerus to the distal metaphysis, with no involvement of the distal forearm structures. Which of the following structures must have been damaged to cause this diffuse bone necrosis?
A 24-year-old woman comes to the physician for an annual routine examination. Menses occur at regular 28-day intervals and last for 4 days with normal flow. Her last menstrual period was 3 weeks ago. She is sexually active with one male partner and they use condoms consistently. The patient is 160 cm (5 ft 3 in) tall and weighs 72 kg (150 lb); BMI is 28.1 kg/m2. She feels well. Pelvic examination shows a smooth, mobile right adnexal mass. A subsequent ultrasound of the pelvis shows a single, 2-cm large, round, hypoechoic mass with a thin, smooth wall in the right ovary. The mass has posterior wall enhancement, and there are no signs of blood flow or septae within the mass. Which of the following is the most appropriate next step in management?
An investigator is studying neuronal regeneration. For microscopic visualization of the neuron, an aniline stain is applied. After staining, only the soma and dendrites of the neurons are visualized, not the axon. Presence of which of the following cellular elements best explains this staining pattern?
Practice by Chapter
Cell structure and organelles
Practice Questions
Microscopy techniques
Practice Questions
Tissue preparation and staining
Practice Questions
Basic tissue types overview
Practice Questions
Cell and tissue identification keys
Practice Questions
Histology of blood and hematopoiesis
Practice Questions
Aging-related histological changes
Practice Questions
Histopathological changes in common diseases
Practice Questions
Immunohistochemistry
Practice Questions
Electron microscopy in histology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app