
CNS Infections — MCQs

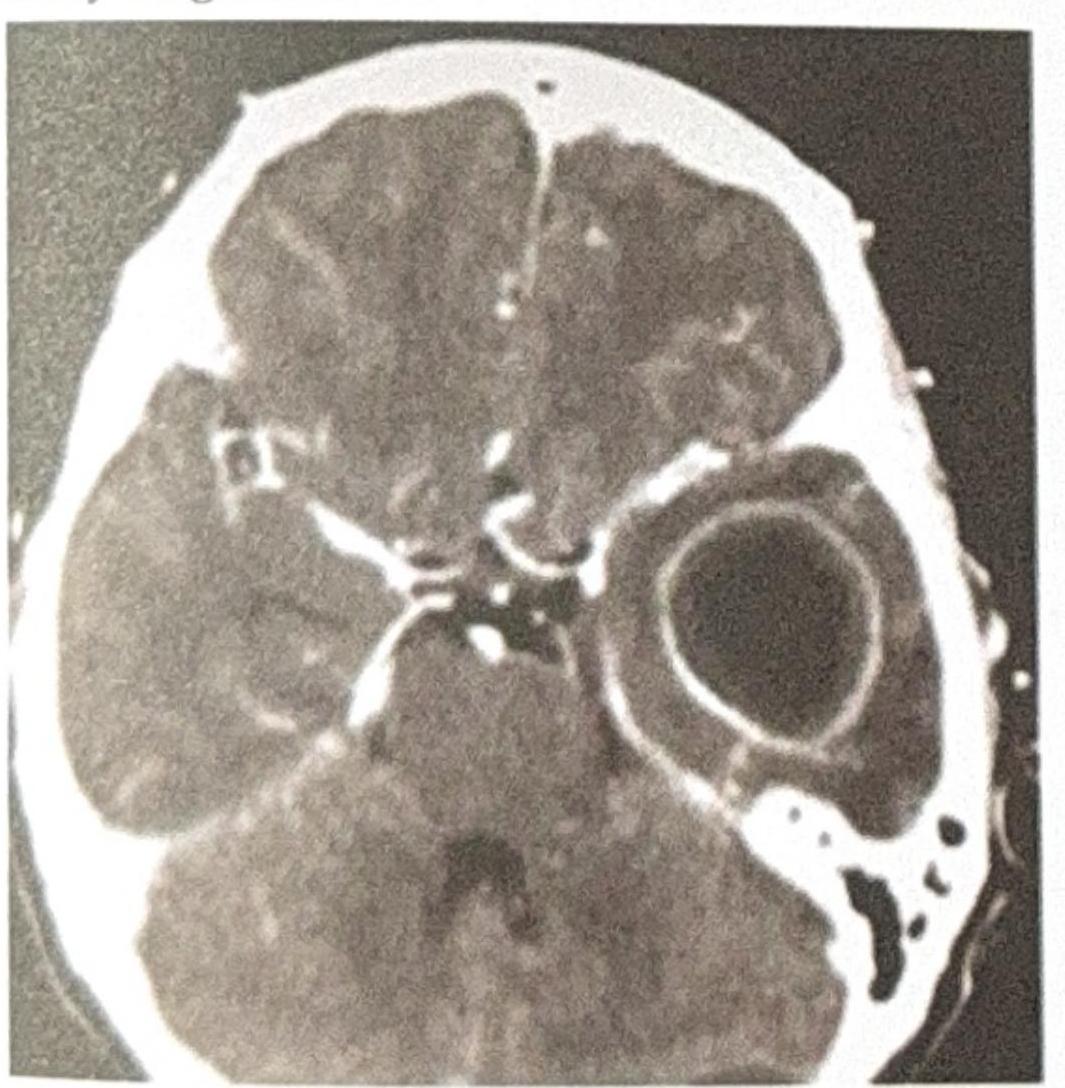
A patient presents with ear discharge. The CT image is shown below. Based on the clinical presentation and imaging, what is the most likely diagnosis?
An 34-year-old male HIV patient on c-A presents with seizures and a unilateral facial nerve palsy. The CT scan shows a ring-enhancing lesion. What is the best treatment?

Symptomatic neonatal CNS involvement is most commonly seen in which group of congenital intrauterine infections?
All of the following statements are true regarding central nervous system infections, except:
Which of the following statements is true regarding HSV encephalitis?
A leukemia patient who has undergone multiple courses of chemotherapy develops herpes simplex encephalitis. Which of the following would you expect a CT scan of the patient's brain to show?
A 65-year-old diabetic man presents with black necrotic tissue on his palate. What is the most likely causative organism?
Which of the following is the MOST COMMON fungal cause of Mucormycosis?
A 40-year-old male presents with a history of headaches, fever, and new-onset seizures. An MRI of the brain is performed, revealing a ring-enhancing lesion with central restricted diffusion on diffusion-weighted imaging (DWI). What is the most likely diagnosis?
Which of the following conditions is most commonly associated with the "doughnut" sign seen on a brain scan?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app