
Abdominal and Pelvic Radiology — MCQs

On this page
What condition is suggested by the below X-ray?

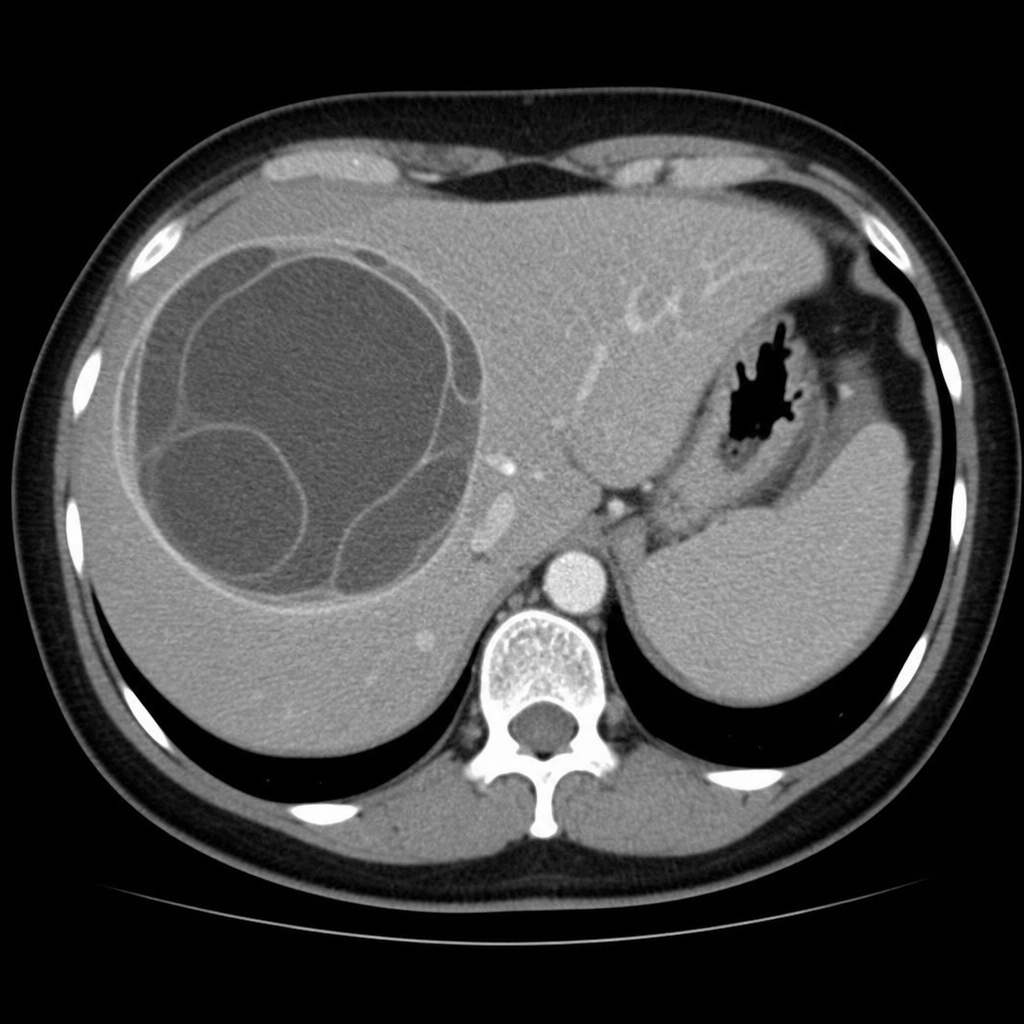
A middle-aged female presents with chronic right-sided abdominal pain and intermittent fever. Clinical examination revealed mild hepatomegaly, and a contrast-enhanced CT abdomen was performed. Based on the imaging characteristics of this focal lesion, what is the most likely diagnosis?
Air in the biliary tract is seen in all of the following conditions except:
Which radiological method is best for staging cervical carcinoma?
Carman's meniscus sign is diagnostic of –
The 'diamond sign' is radiographically observed in which of the following conditions?
A patient with a history of choledocholithiasis presents with elevated conjugated bilirubin. Ultrasound reveals a dilated biliary system up to the terminal pancreas. In case of suspicion of an ampullary obstructive calculus, which of the following investigations would be most sensitive?
A barium swallow shows which of the following findings?

Endometriomas on ultrasound typically appear as?
In a pregnant woman of 28 weeks gestation, intrauterine fetal death (IUD) is earliest demonstrated on X-ray by which sign?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app