
Abdominal and Pelvic Radiology — MCQs

On this page
Which of the following is true regarding the principles of MRCP?
A plain radiograph of a patient with chronic abdominal pain is provided. What is the probable diagnosis based on the image?

A patient presents with right hypochondrium pain. Which of the following investigations should be done?
The 'apple core' sign observed in a barium enema is typically associated with which of the following conditions?
Calcific hepatic metastases are most commonly seen in which of the following primary tumors?
Which investigation is useful for detecting extraadrenal pheochromocytoma?
What is the term for the appearance of diverticulosis on a barium enema as depicted in the image?

Tear drop bladder is seen in which of the following conditions?
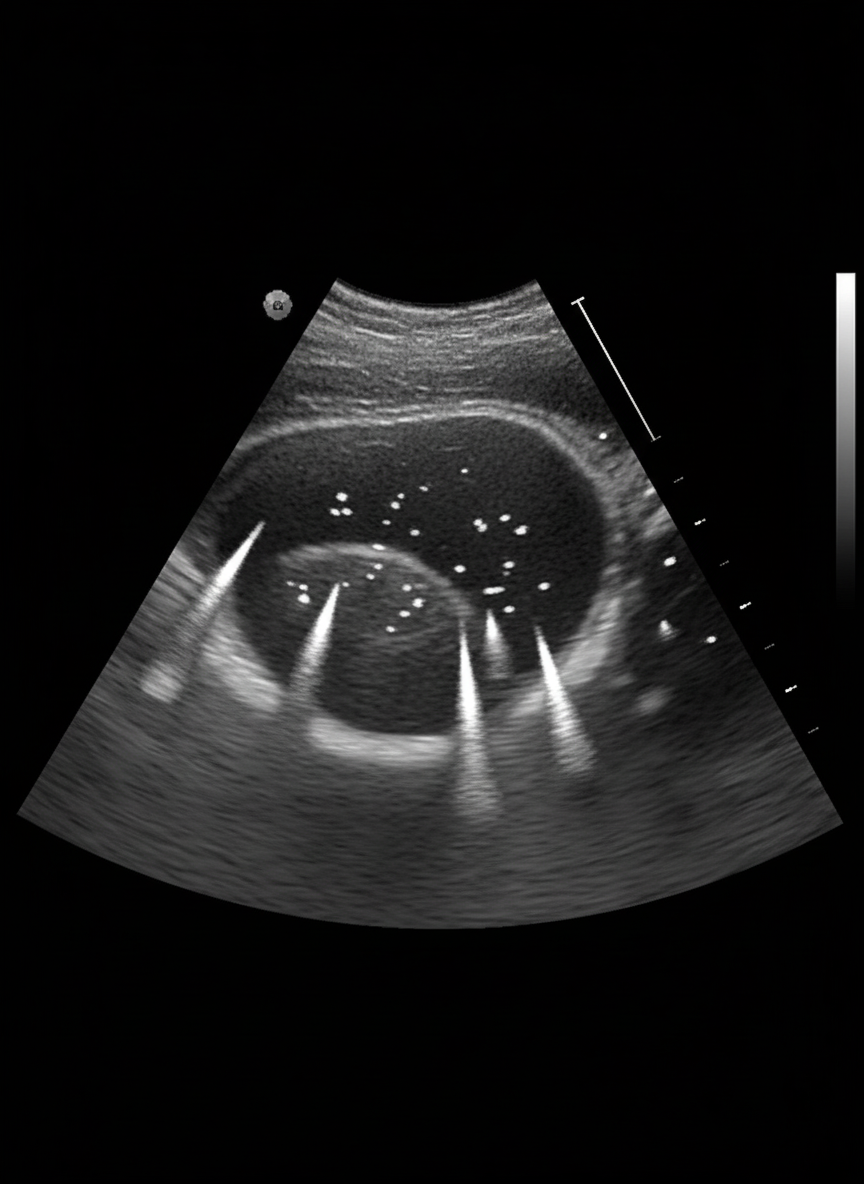
An incidental finding on ultrasound abdomen is suggestive of which of the following?
A 45-year-old male shows calcification on the right side of his abdomen in an AP view. In the lateral view, the calcification is seen to overlie the spine. What is the most likely diagnosis?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app