
Abdominal and Pelvic Radiology — MCQs

On this page
Which imaging modality is considered the best for staging rectal carcinoma?
The most appropriate first-line investigation to be performed in suspected cases of gastric cancer is:
Which of the following HSG findings is most suggestive of genital tuberculosis?
Which of the following is a direct (primary) sign of obstruction of the urinary tract on a CT scan?
Investigation of choice for detecting hepatic metastasis from stomach cancer is
The 'coffee bean sign' is typically seen in which condition?
Which of the following is a radiological sign of acute pancreatitis on plain radiography?
Depth of gastric carcinomas is assessed by -
What is the most sensitive investigation for detecting minimal gas in the abdomen?
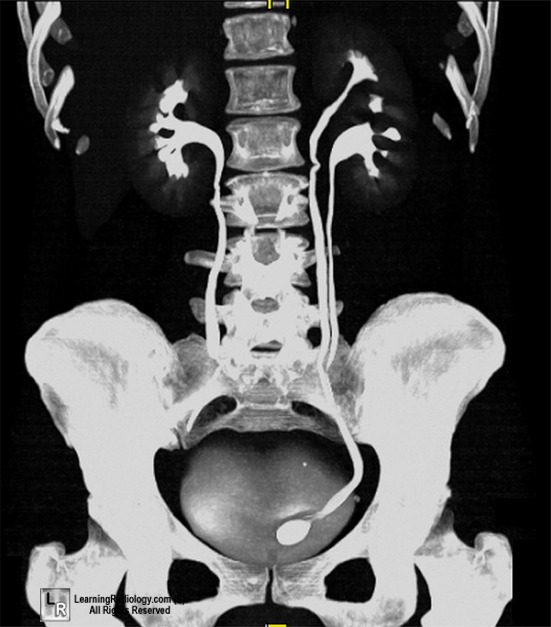
A female patient presented with recurrent urinary tract infections. Imaging shows the following picture. What can be the most probable diagnosis based on the imaging findings?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app