
Abdominal and Pelvic Radiology — MCQs

On this page
Radio-lucent renal stones are typically composed of which substance?
Which of the following is the most specific and sensitive screening test for renovascular hypertension?
A patient with abdominal pain shows a "coffee bean" sign in a plain abdominal X-ray. What is the probable diagnosis?
Non-visualization of the gastric fundic bubble with an air-fluid level in the retrocardiac region suggests which of the following?
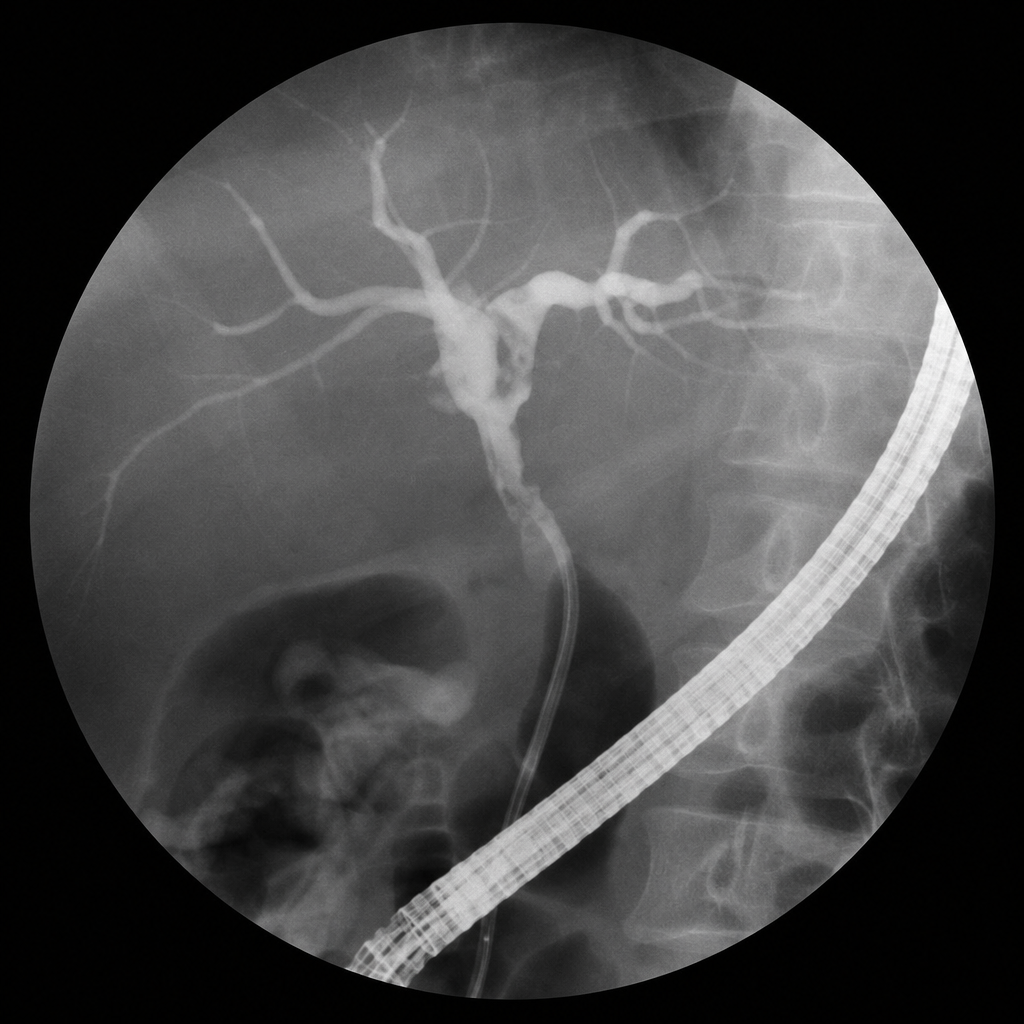
What does the cholangiogram show?
The 'bowler hat' sign is radiographically observed in which of the following conditions?
What does the term "pseudo kidney" refer to in medical imaging?
Multiple air-fluid levels in a child are seen in which condition?
Which of the following are true features of cholecystitis on ultrasonography?
Which of the following liver metastases appear hypoechoic on ultrasound?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app