
Abdominal and Pelvic Radiology — MCQs

On this page
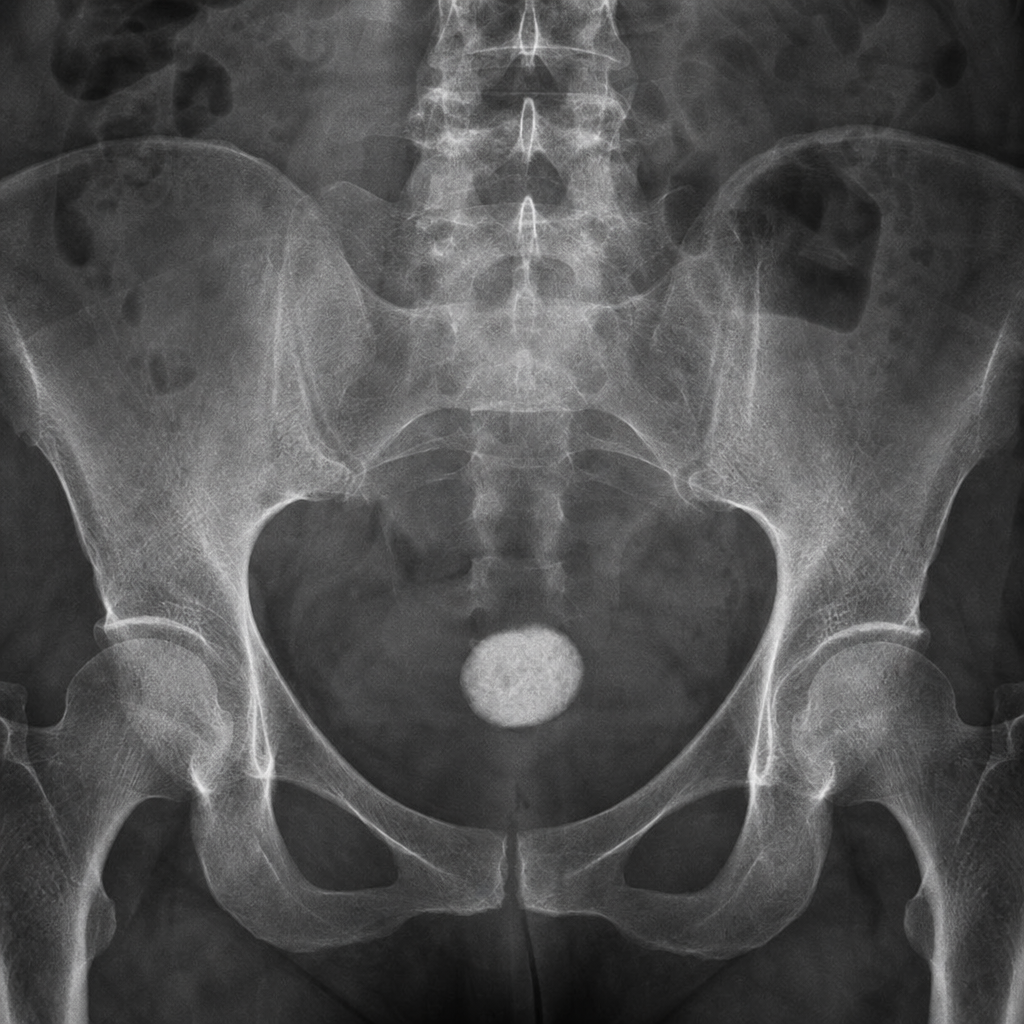
What is the structure seen in the X-ray?

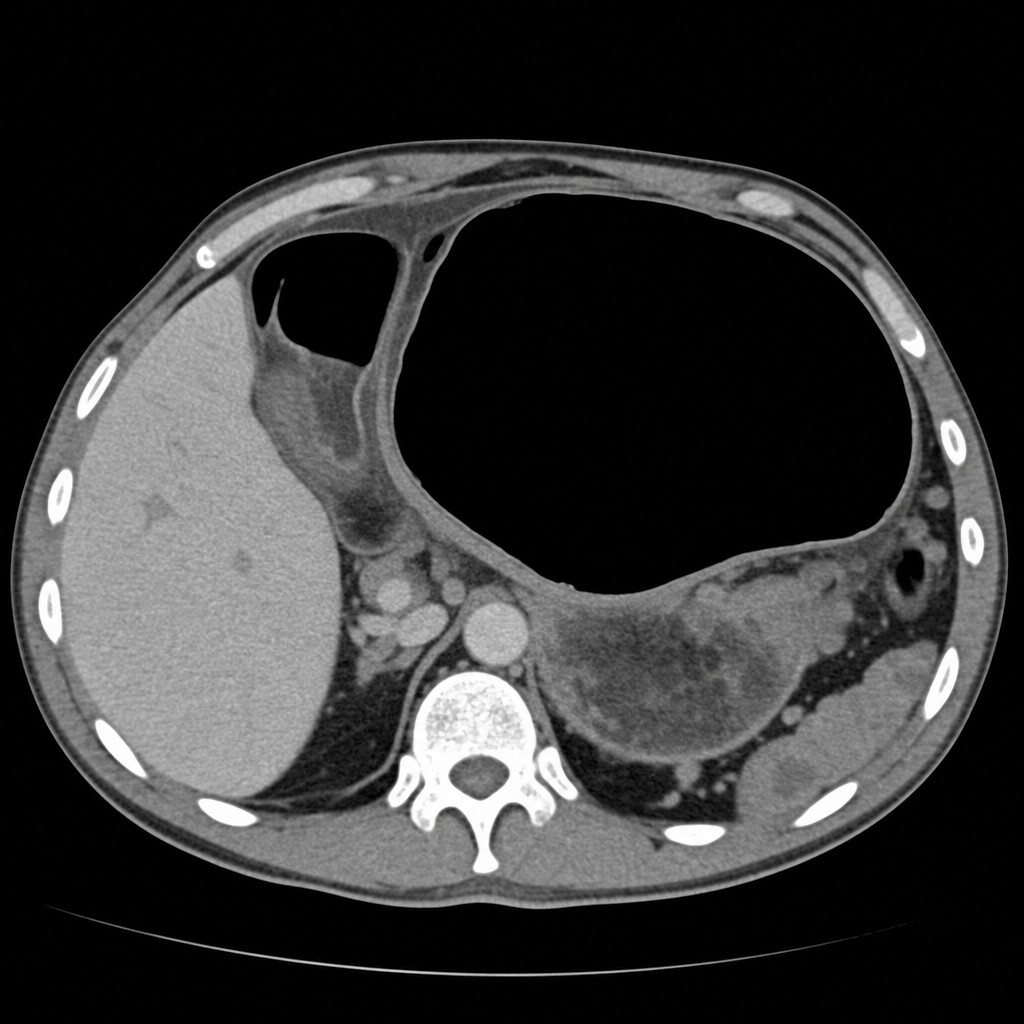
On CT scan, gastric volvulus typically shows which of the following findings?
What is the diagnosis based on the following X-ray image?
In a patient with a tender and rigid abdomen, what is the expected finding on X-ray?
Which of the following X-ray findings is associated with Chilaiditi syndrome?
Cobra head appearance on excretory urography is suggestive of?
Rigler's sign is suggestive of?
What is the best investigation for diagnosis and staging of renal cell carcinoma with thrombus extending into the IVC?
Which of the following imaging modalities is most appropriate for initial evaluation of suspected acute appendicitis in a young adult patient?
"String of beads" appearance on horizontal abdominal view X-ray is suggestive of:
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app