
Abdominal and Pelvic Radiology — MCQs

On this page
The 'coffee bean sign' is typically seen in which condition?
Mercedes Benz sign is seen in:
Christmas tree appearance of urinary bladder is seen in
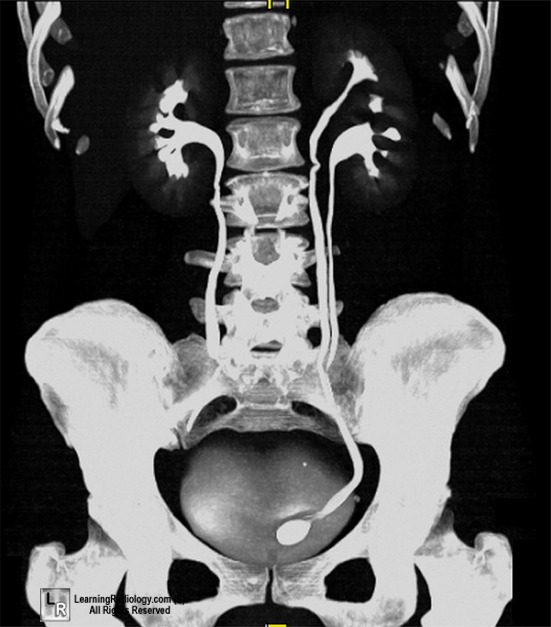
A delayed intravenous urogram of a patient is given below. What is the likely diagnosis?

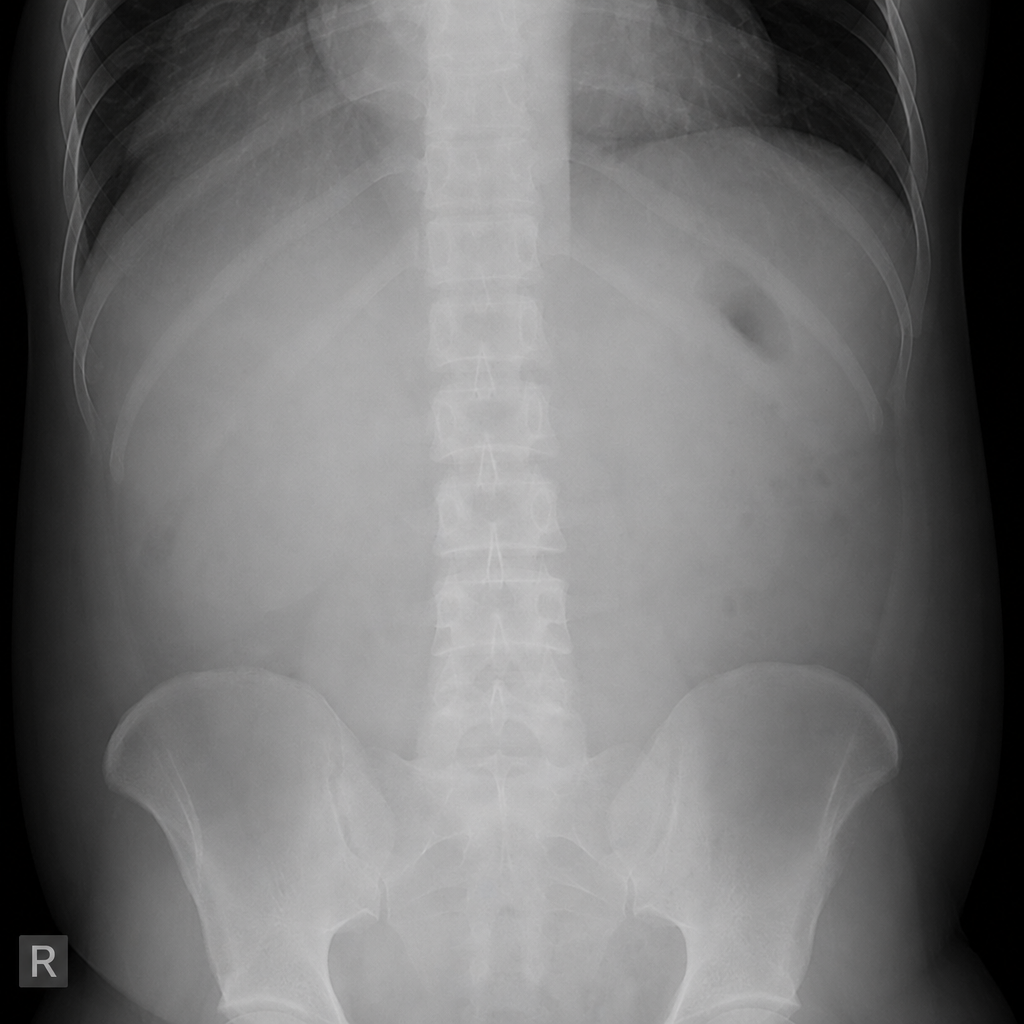
A patient presents with severe epigastric pain, markedly elevated serum lipase, and imaging showing substantial ascites. In this clinical setting, which diagnosis best explains the gasless abdominal radiograph?
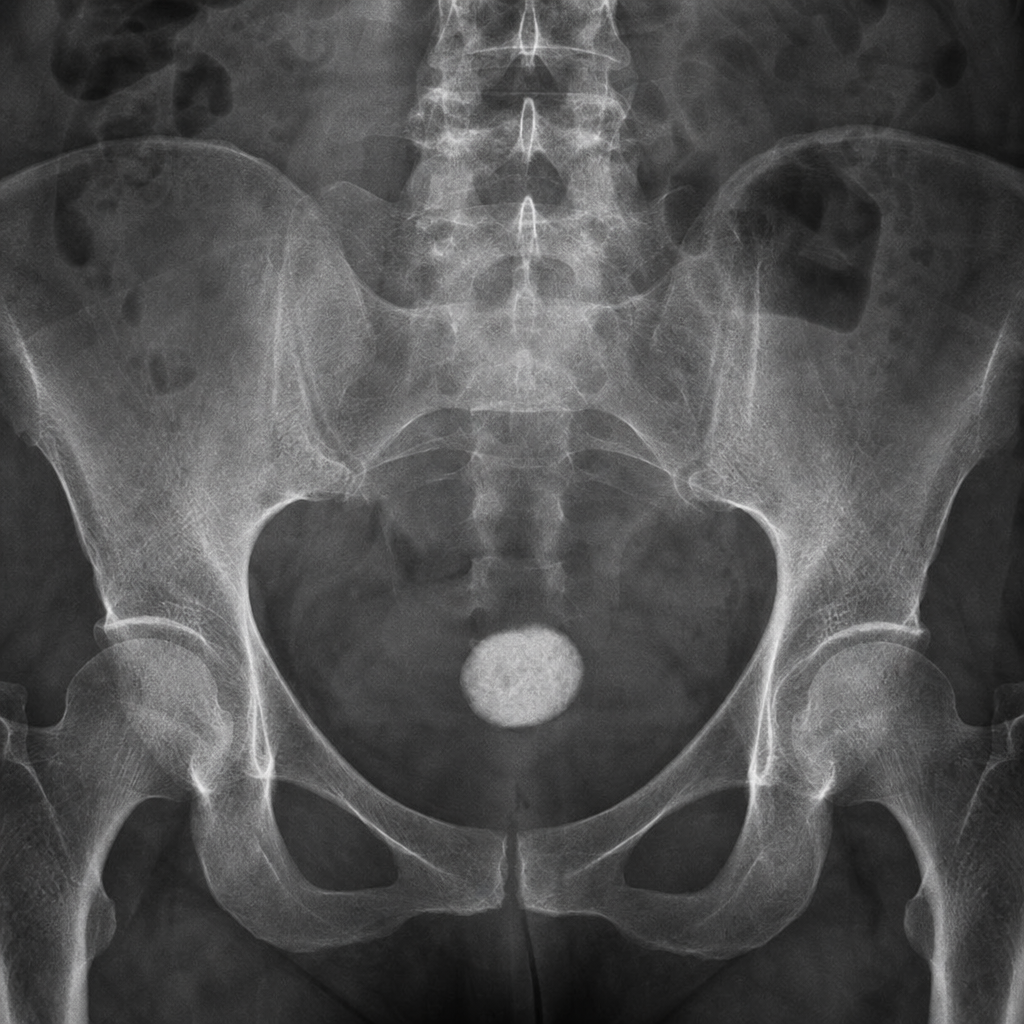
A female patient presented with recurrent urinary tract infections. Imaging shows the following picture. What can be the most probable diagnosis based on the imaging findings?
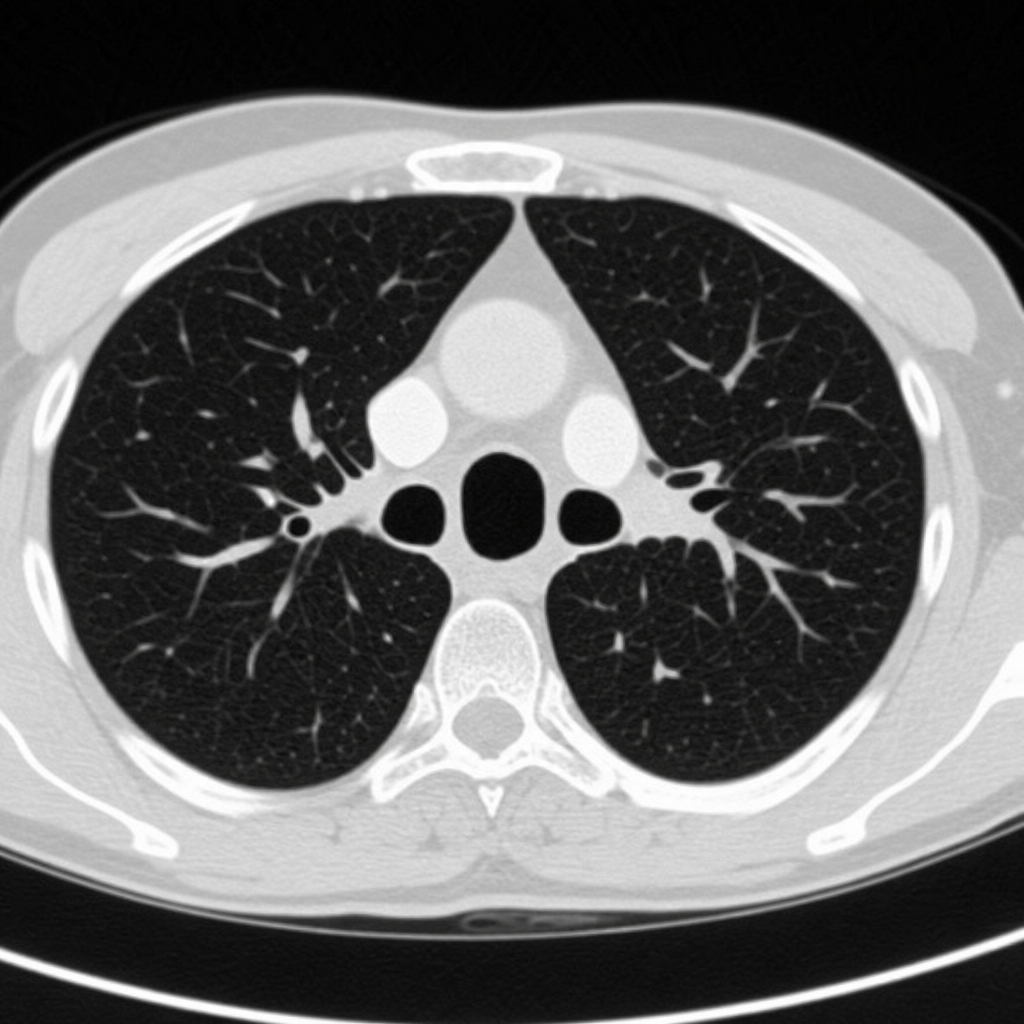
Which radiological finding is shown in the image?

What does the sign depicted in the image represent?
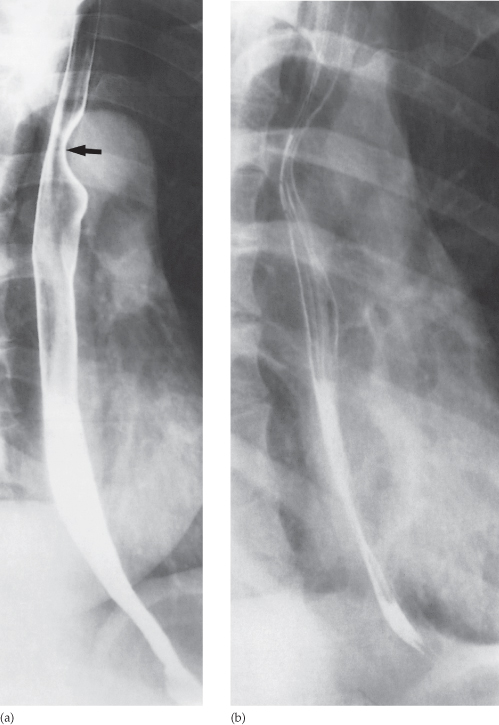
The Barium Swallow examination shows a mass in the esophagus. What can be the most probable diagnosis?
What is the diagnosis based on the following X-ray image?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app