
Abdominal and Pelvic Radiology — MCQs

On this page
A 75-year-old male with a history of hypertension presents with sudden-onset severe abdominal pain radiating to the back. Which diagnostic tool would be most beneficial in differentiating between a ruptured abdominal aneurysm and acute pancreatitis?
What does the 'football sign' on an abdominal X-ray indicate?
The Barium Swallow examination shows a filling defect in the esophagus. What is the most probable diagnosis?
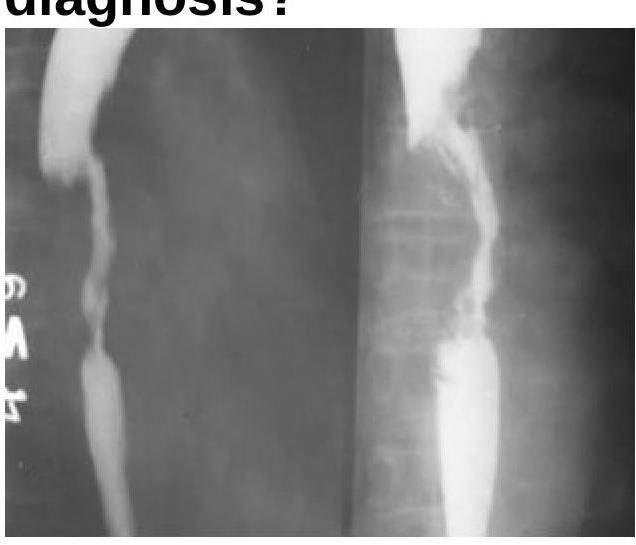
Identify the radiological sign of Ischemic colitis from the image provided.
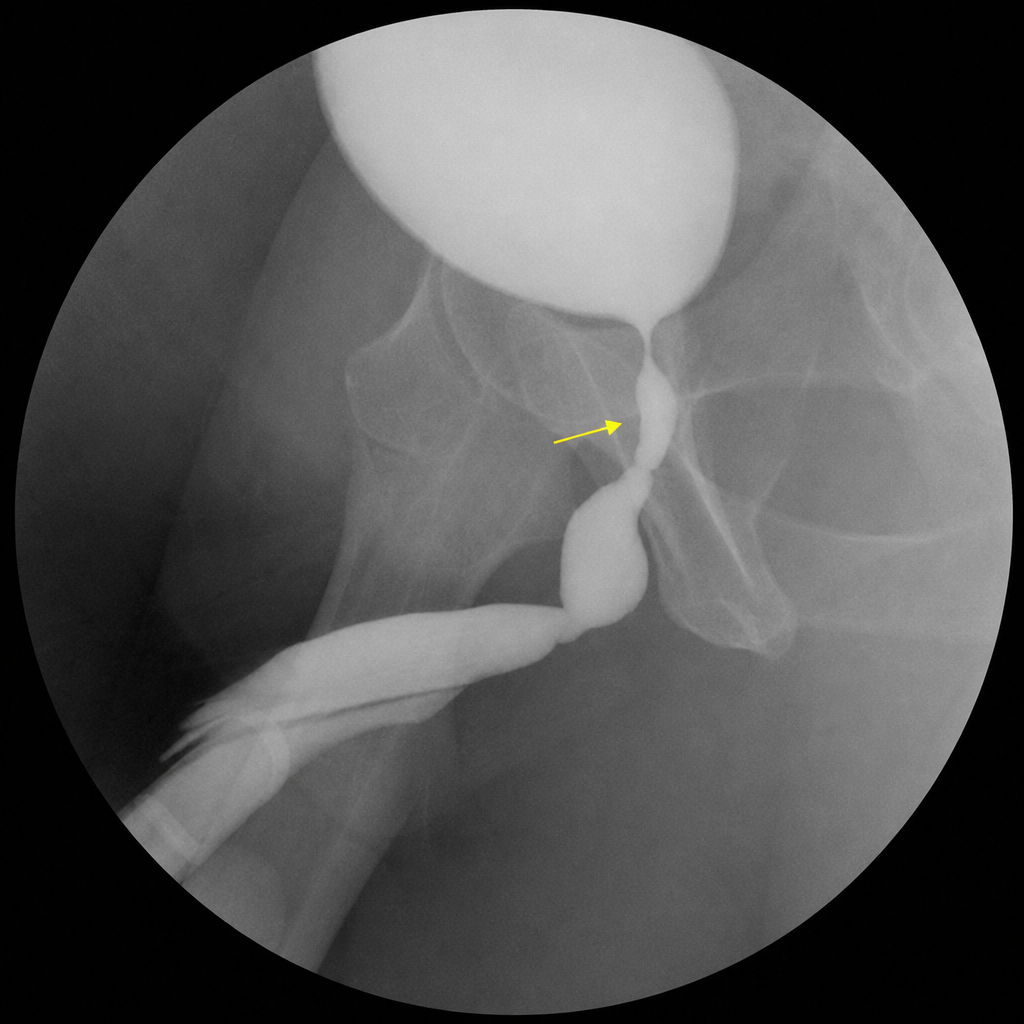
A female patient presented with recurrent urinary tract infections. What is the most probable diagnosis based on the imaging findings?

Based on the imaging findings, identify the condition associated with the following results.
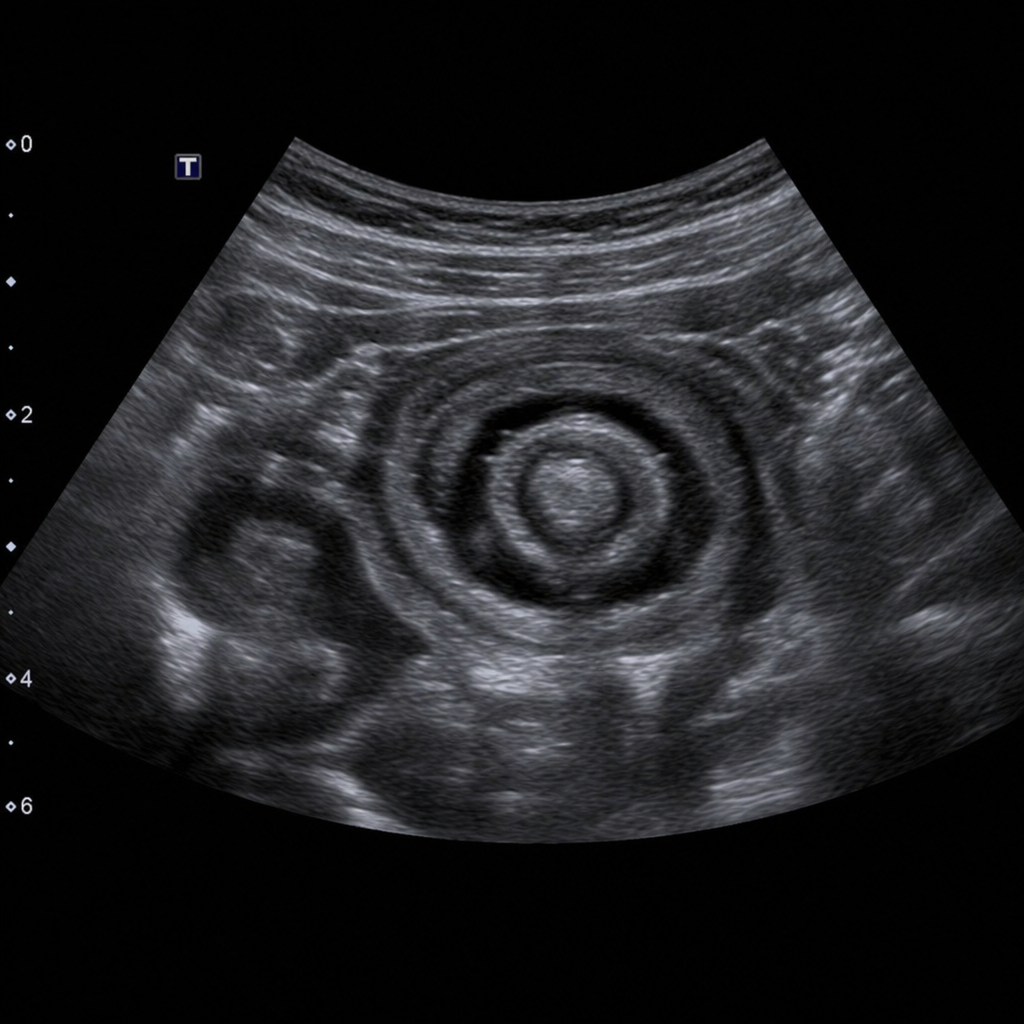
What radiological sign is depicted in this ultrasound image?
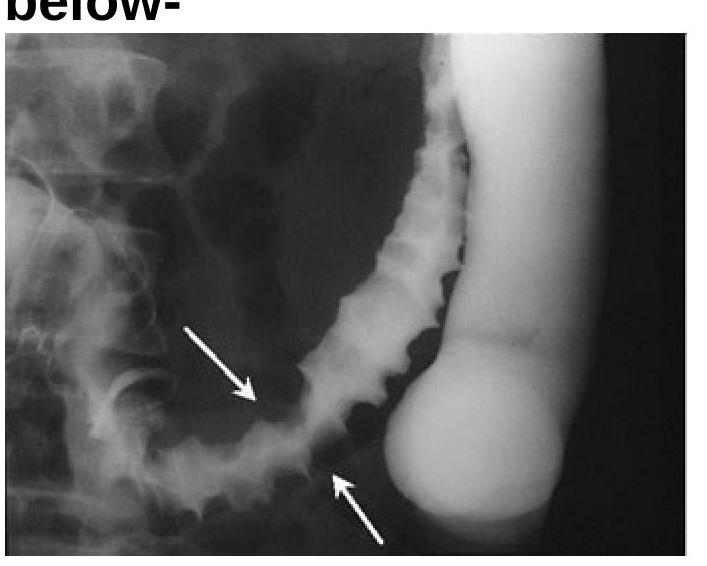
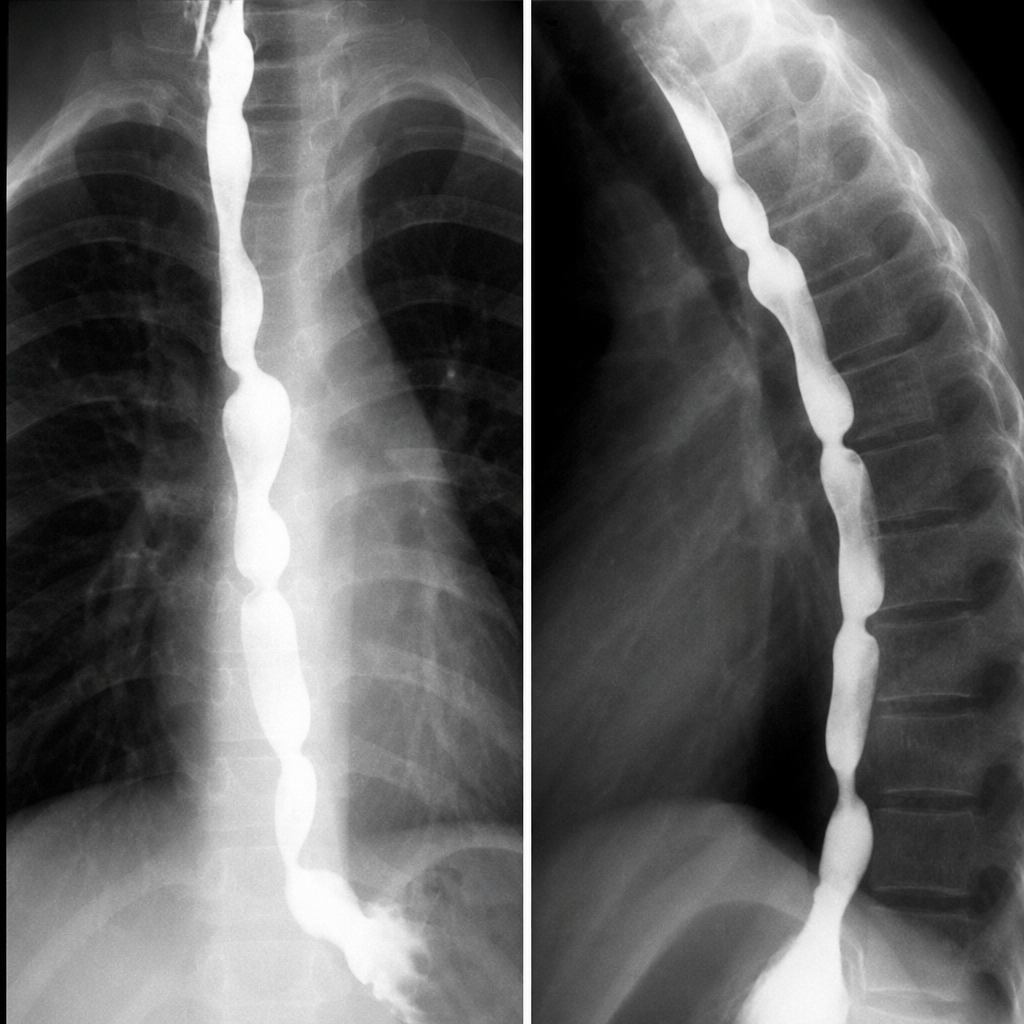
What does the following radiograph from a double contrast esophagram represent?
A 35-year-old patient with weight loss, sterile pyuria, and a history of pulmonary tuberculosis undergoes a plain abdominal radiograph. It shows irregular, dense calcification conforming to the right renal outline in the renal fossa, consistent with extensive dystrophic calcification of the kidney. What is the most likely diagnosis?

Which condition is associated with the "Drooping lily sign"?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app