
Abdominal and Pelvic Radiology — MCQs

On this page
Double decidual sac sign is indicative of?
In which of the following conditions is air under both sides of diaphragm visualized -
Claw sign seen in?
USG findings of focal anechoic lesion with floating membranes indicate which liver pathology?
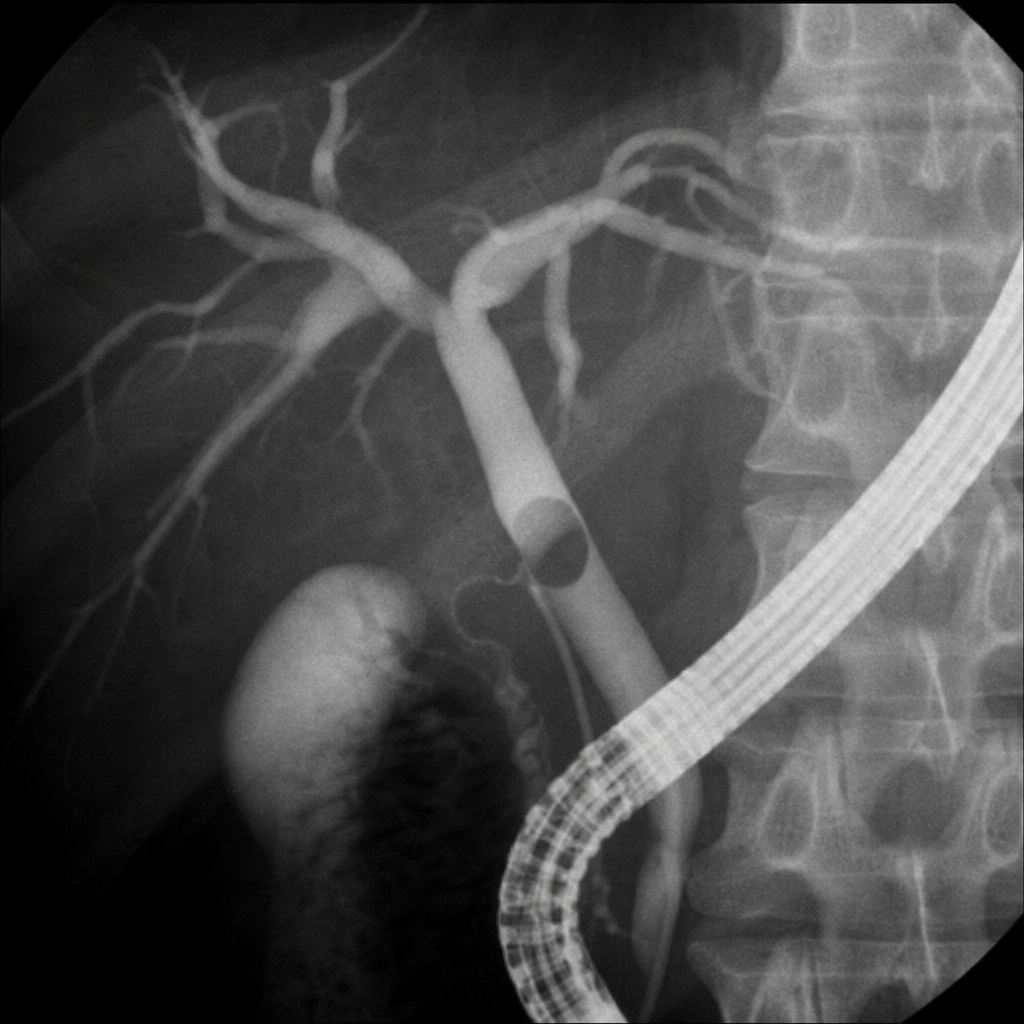
X-Ray appearance of CBD stone on cholangiography is:
Gas absent from intestine (gasless abdomen) on x-ray is seen in which condition?
Causes of thickened gallbladder wall on ultrasound examination are all except:
A dense persistent nephrogram may be seen in all of the following except:
A patient with right lower quadrant pain shows target sign on ultrasound. Diagnosis?
What is the characteristic feature of hepatocellular carcinoma on triphasic CT?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app