
Abdominal and Pelvic Radiology — MCQs

On this page
The best investigation for air in the peritoneal cavity is:
In which of the following conditions is the lead pipe appearance of the colon seen on a barium enema?
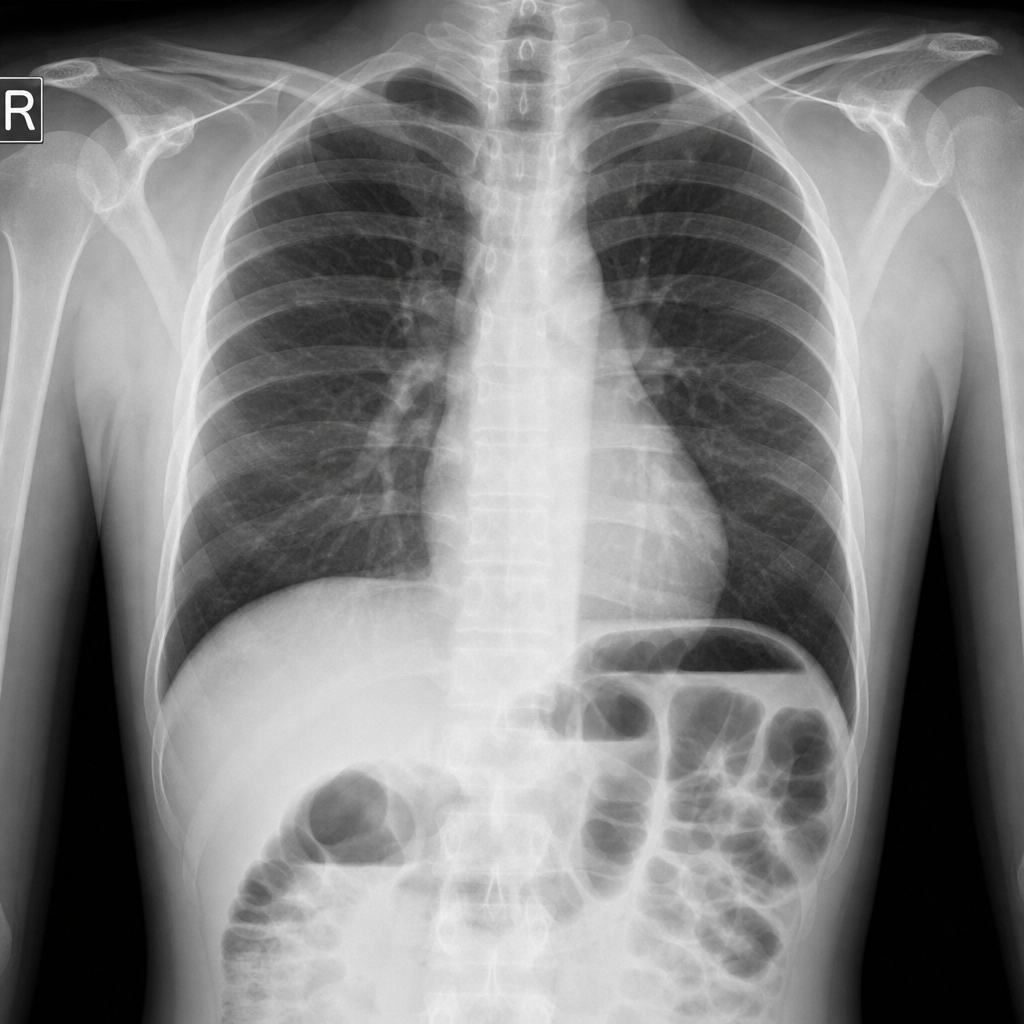
X-ray given below suggestive of:
Which of the following liver metastases appear hypoechoic on ultrasound?
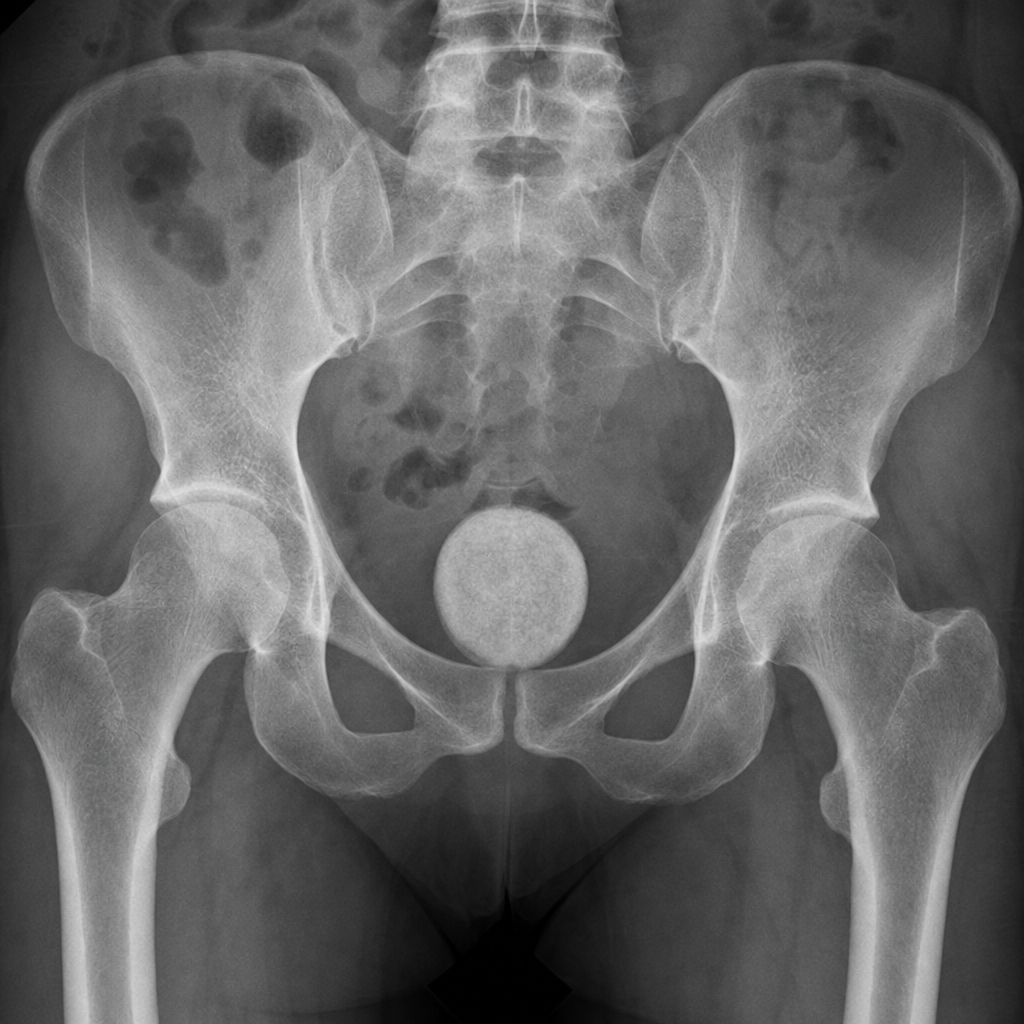
What is the diagnosis based on the following X-ray?
Focal and diffuse thickening of gallbladder wall with high amplitude reflections and 'comet tail' artifacts on USG suggest the diagnosis of –
All are sonological features of Budd Chiari syndrome, EXCEPT:
What is the structure seen in the given X-ray below?

All are important ultrasound findings of amebic liver abscess, EXCEPT:
The "Target sign" ultrasonographically means:
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app