
Abdominal and Pelvic Radiology — MCQs

On this page
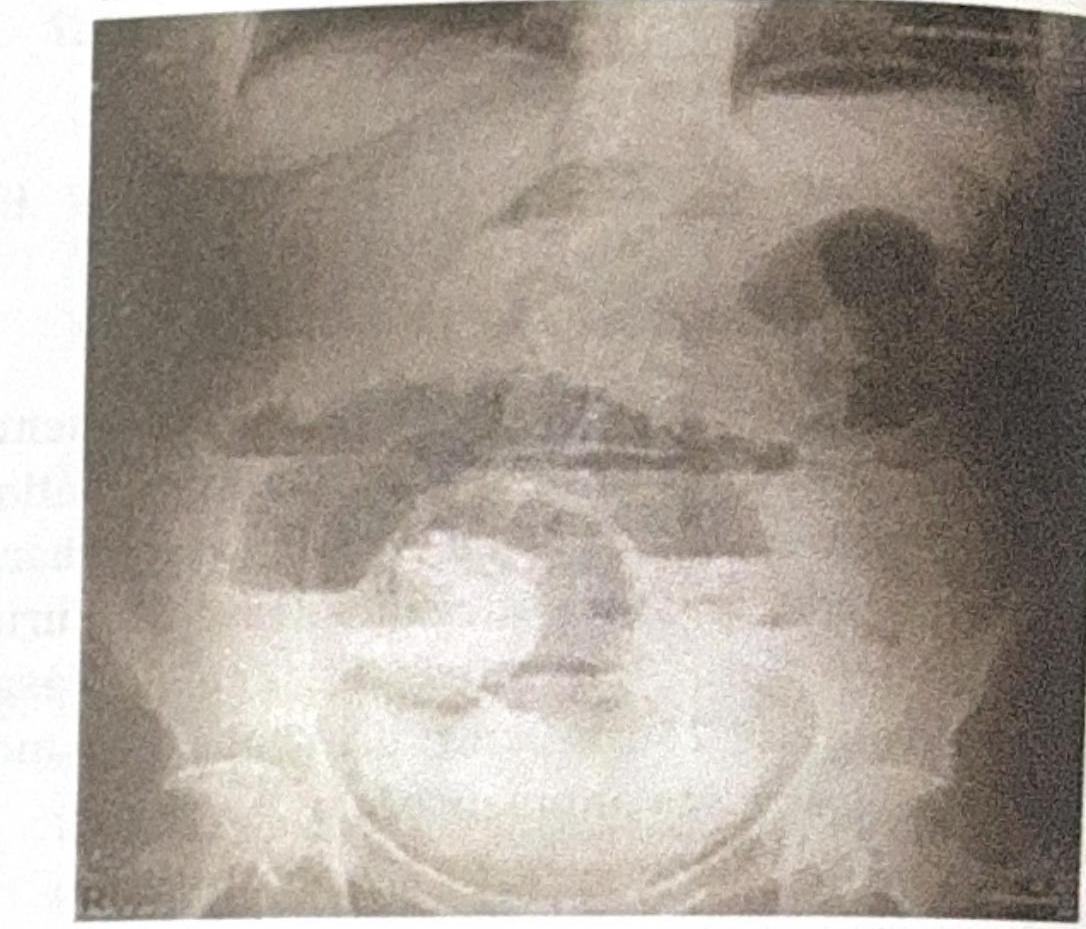
A patient presents with abdominal distension. Based on the X-ray, which of the following bowel loops are dilated?

Examine the abdominal X-ray shown. What is the most likely diagnosis based on the findings?
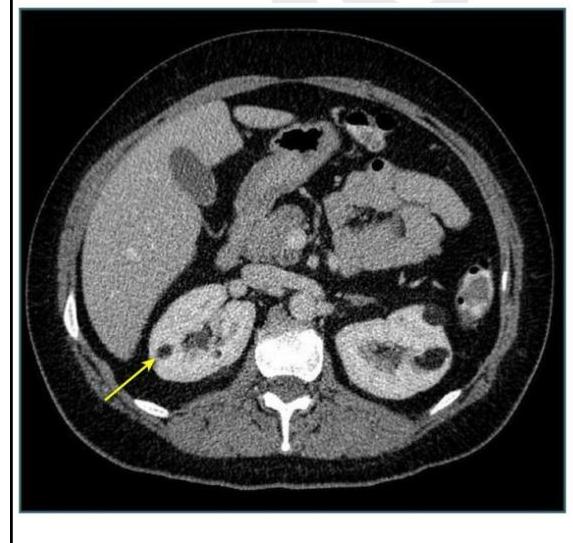
Identify the condition based on the non-contrast CT scan of a patient given below.

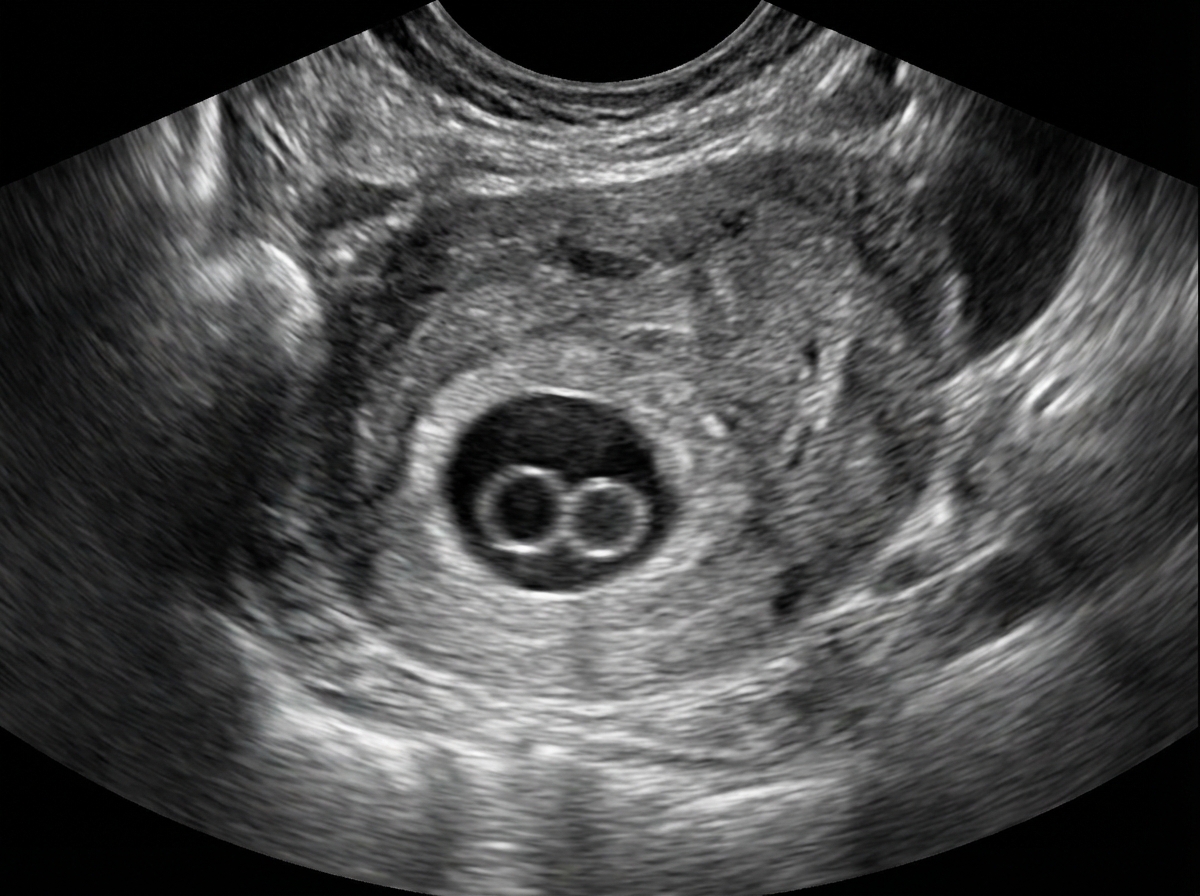
Double bleb sign seen in early pregnancy is due to?
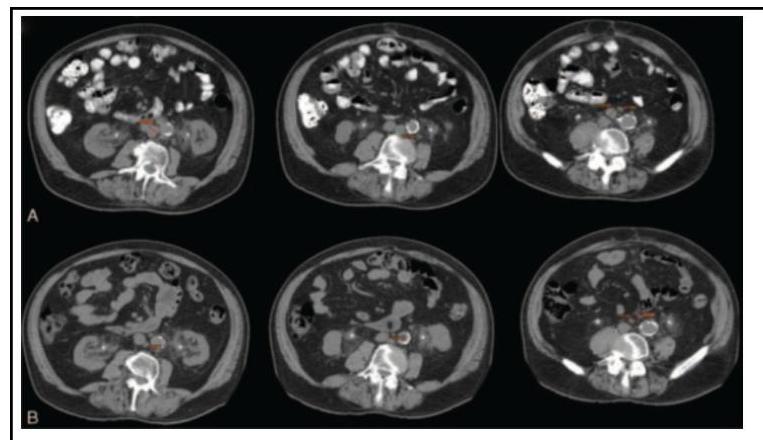
A 45-year-old patient presented with vague abdominal pain. On USG, he was found to have a renal cyst of Bosniak class III. CECT was done, as shown below. What imaging modality is shown?
During rounds, your senior was discussing the given image. Which of the following investigations does this image represent?
Double decidual sign is seen in?
Which of the following is a gold standard investigation for diagnosis of renal stone?
Pulsatile Doppler signal (continuous flow) in the hepatic vein in the setting of Budd-Chiari syndrome indicates:
One of the following is characterised by RIM sign?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app