
Abdominal and Pelvic Radiology — MCQs

On this page
Among the following, which is the investigation of choice for evaluation of common bile duct (CBD)?
Consider the following radiological signs : 1. Claw sign in barium enema 2. Apple core sign in barium enema 3. Multiple fluid levels with absent caecal gas in plain skiagram of abdomen 4. Single large fluid and air level in plain skiagram of abdomen Which of the above signs is/are suggestive of ileocolic intussusception?
'Double duct' sign is diagnostic of
A 20 years old man had history of pain in the right side of abdomen. His X-ray abdomen AP view shows radio-opaque shadow, which on lateral film falls behind the vertebral column. The probable diagnosis is:
'Chain of Lakes' appearance due to sacculation with intervening short strictures of pancreatic duct is seen on:
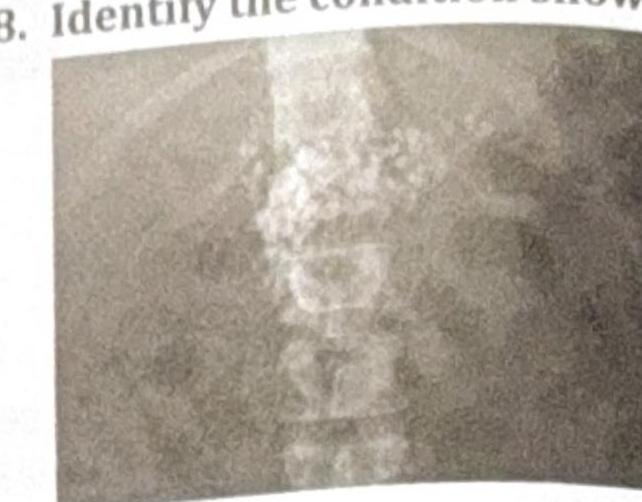
Identify the condition shown in the plain abdominal radiograph.
A 45-year-old farmer presents with right upper quadrant pain and a history of exposure to livestock. An abdominal ultrasound shows a cystic lesion in the liver with internal floating membranes, described as the "Water lily sign." Based on this finding, what is the most likely Gharbi classification stage of the hydatid cyst?

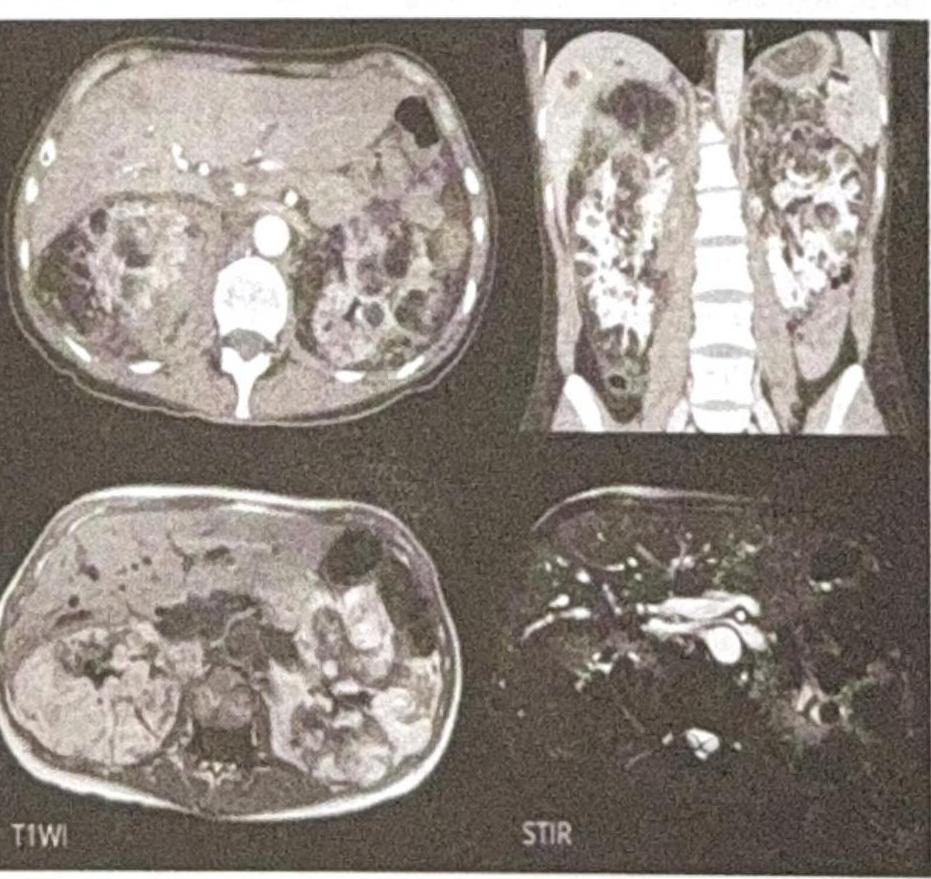
What is the Diagnosis based on the CT and MRI images given below?
A 28-year-old woman presents with recurrent right upper quadrant pain and jaundice since childhood. The MRCP image shows a large cystic dilation of the extrahepatic bile duct with no distal obstructing lesion, no calculi, and no stricture identified. What condition does the MRCP (Magnetic Resonance Cholangiopancreatography) image indicate?

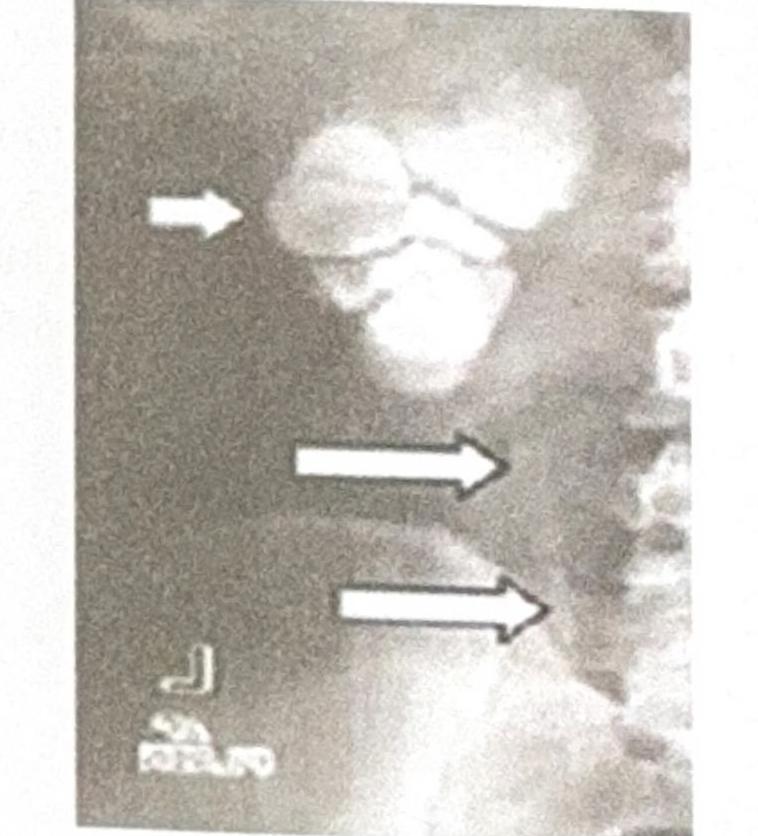
A 30-year-old female presents with sterile pyuria. The radiograph below is provided. What is the most likely diagnosis?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app