
Abdominal and Pelvic Radiology — MCQs

On this page
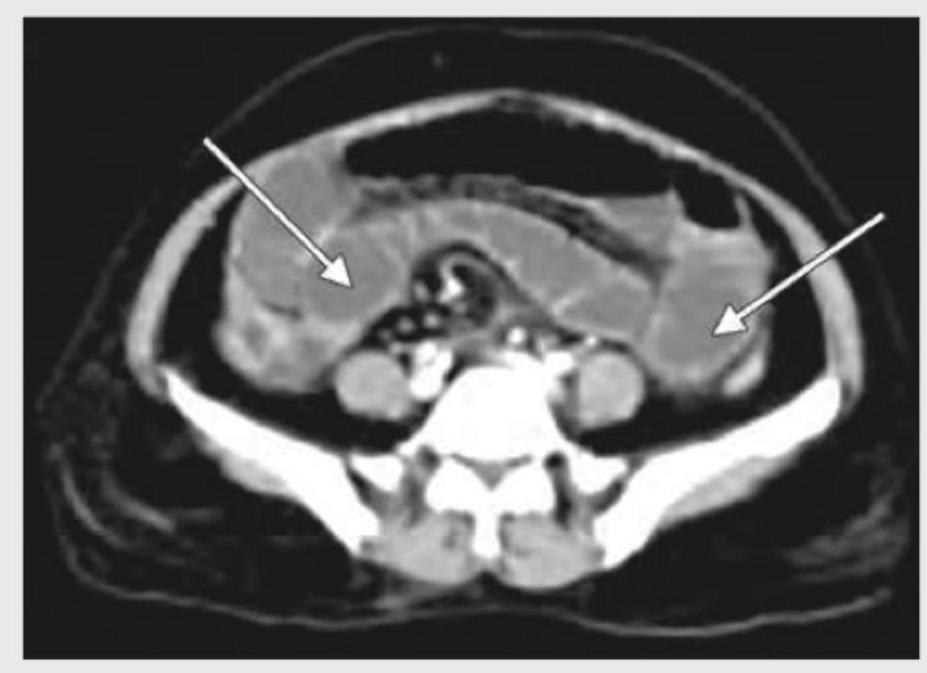
Identify the condition shown in the figure:
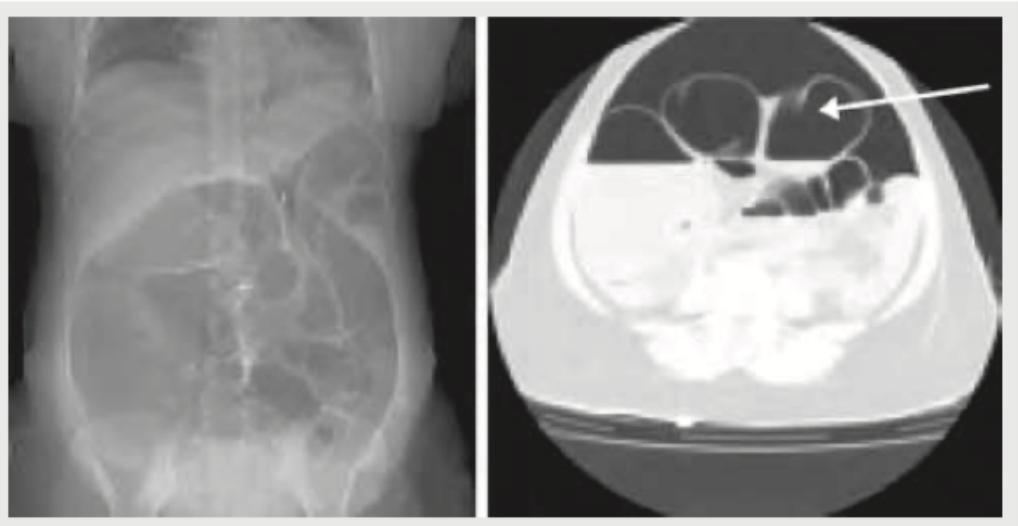
A 30-year-old male presents with acute abdomen. What radiologic finding is demonstrated on the CT abdomen given below?
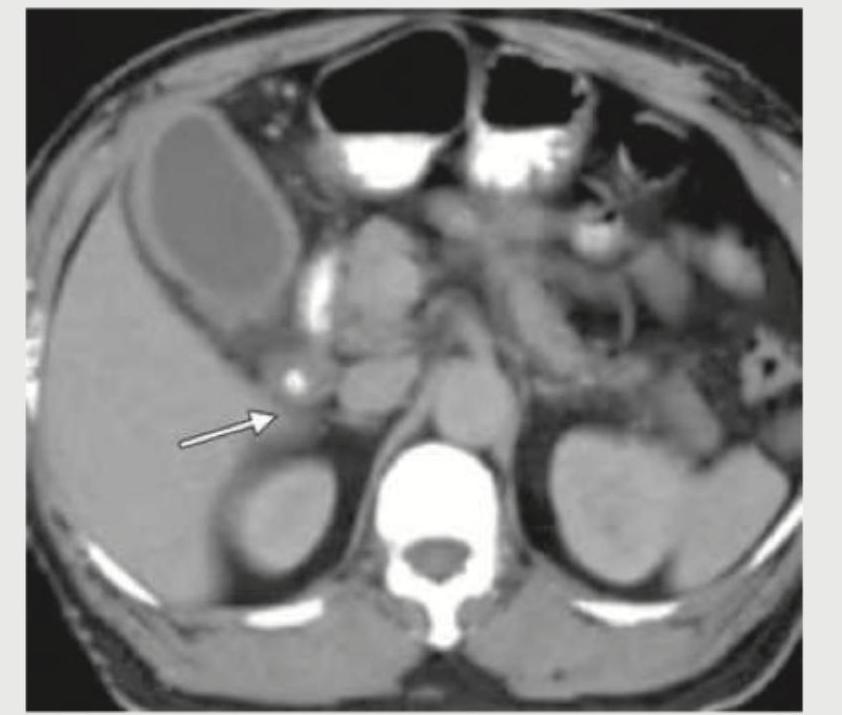
Identify the lesion shown in the figure:
What is the radiological sign demonstrated in the image provided?
Which of these is best for imaging an indeterminate solid renal mass in the kidney of a 60-year-old man with normal renal function and no contraindication to iodinated contrast?

Comment on the diagnosis of the image shown below.

A 32-year-old lady presents with history of first trimester miscarriage and underwent HSG. Examination reveals a single cervix, and MRI confirms a single uterine horn. The diagnosis is: (Recent NEET Pattern 2018-19)

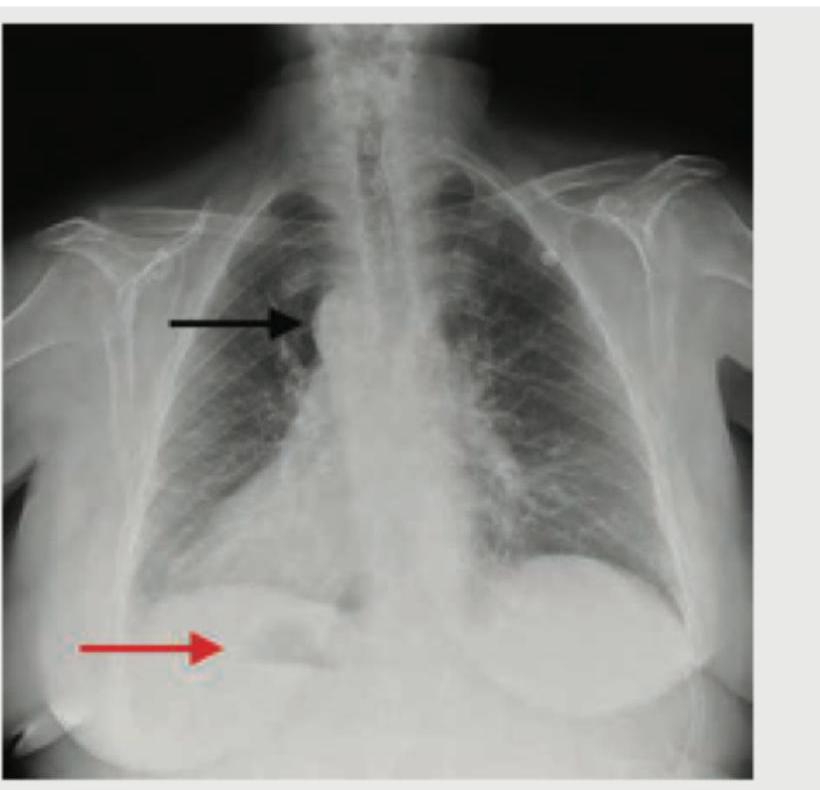
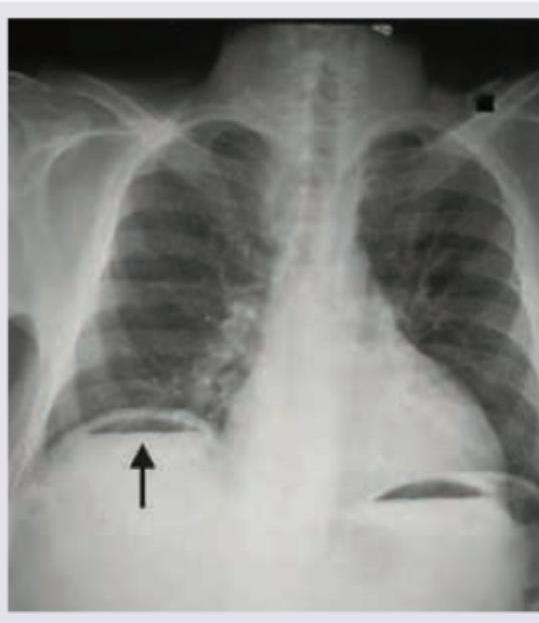
What does the given chest X-ray show?
The first imaging modality of choice for a 35-year-old lady, presenting to surgical emergency with complaints of colicky pain in right lower quadrant of abdomen and vomiting since last 2 days is:
The 'claw sign' in barium enema study favours the diagnosis of :
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app